
The court further prohibited Kenya from admitting or facilitating the entry of Ebola-exposed persons under the arrangement in which the US was spending $1.7 billion for a 50-bed quarantine facility in Nanyuki.
The High Court in Nairobi has temporarily blocked the Kenyan government from establishing a United States-linked Ebola quarantine facility in the country, following a petition raising constitutional and public health concerns.
Justice Patricia Nyaundi issued conservatory orders barring the government from establishing, operationalising, facilitating or approving any Ebola exposure, quarantine, isolation or treatment facility linked to the United States or any foreign government, pending the hearing and determination of the case. The court also prohibited Kenya from admitting or facilitating the entry of persons exposed to or infected with Ebola under the disputed arrangement. The case will be mentioned on June 2, 2026.

The orders were granted following a petition by Katiba Institute, which sued the Attorney General and the Ministry of Health, arguing that the alleged Kenya-US agreement was being pursued secretly and without constitutional safeguards, including public participation and parliamentary oversight.
“The impugned arrangement is being undertaken in a manner that is not transparent and is devoid of constitutional accountability, public participation, parliamentary oversight or full disclosure of its health, environmental, and security implications,” Katiba Institute stated.
US government pledged about Ksh1.7 billion towards Kenya’s Ebola preparedness
The proposed facility was reportedly set to be established at the Laikipia Air Base in Nanyuki. Under the arrangement, American citizens exposed to Ebola while working or travelling in outbreak-hit regions would be flown to Kenya for quarantine and monitoring rather than being repatriated directly to the United States.
Those who developed symptoms would then be transferred to European countries for treatment. The US government had pledged about Ksh1.7 billion ($13.5 million) towards Kenya’s Ebola preparedness and the establishment of the proposed 50-bed facility.
Kenya’s Principal Secretary for Medical Services, Dr Ouma Oluga, defended the discussions, saying Kenya’s strategic location, medical infrastructure and experience in handling regional disease outbreaks made it an ideal partner in global health security. “The Kenyan government continues to protect Kenyans, but as we do so, we can’t abdicate our duty in global health security. This is what we are known to do for decades. This is where more than 100 countries send cases for testing,” he said.
The plan nonetheless triggered widespread public backlash, with Kenyans raising concerns over the country’s preparedness to handle highly infectious diseases and fears that Kenya was being turned into a quarantine destination for foreign nationals. The Kenya Medical Practitioners Pharmacists and Dentists Union (KMPDU) demanded full disclosure of the agreement and warned of possible industrial action if the government failed to provide transparency.
The Ministry of Health has also intensified screening procedures, contact tracing preparedness
US Secretary of State Marco Rubio defended the arrangement during a cabinet meeting in Washington. “We cannot and will not allow any cases of Ebola to enter the United States,” he said, adding that the goal was to contain the crisis to the countries where it is currently located.

Health officials have maintained that no Ebola case has been reported in Kenya and that stringent containment measures remain in place, including heightened surveillance at airports and border crossings, particularly for travellers arriving from high-risk countries such as the Democratic Republic of Congo and Uganda. The Ministry of Health (MoH) has also intensified screening procedures, contact tracing preparedness, isolation readiness and laboratory testing capacity in collaboration with the World Health Organization (WHO), Africa CDC and other international partners.
The current outbreak, first declared in the DRC in May 2026, is caused by the Bundibugyo species, a rare variant with no approved vaccine or targeted treatment. The WHO reports more than 1,000 suspected and confirmed infections and over 220 deaths, while other estimates place the figures at more than 1,270 cases and at least 263 deaths. Uganda has confirmed cross-border infections, and health authorities are monitoring possible exposures in South Sudan.
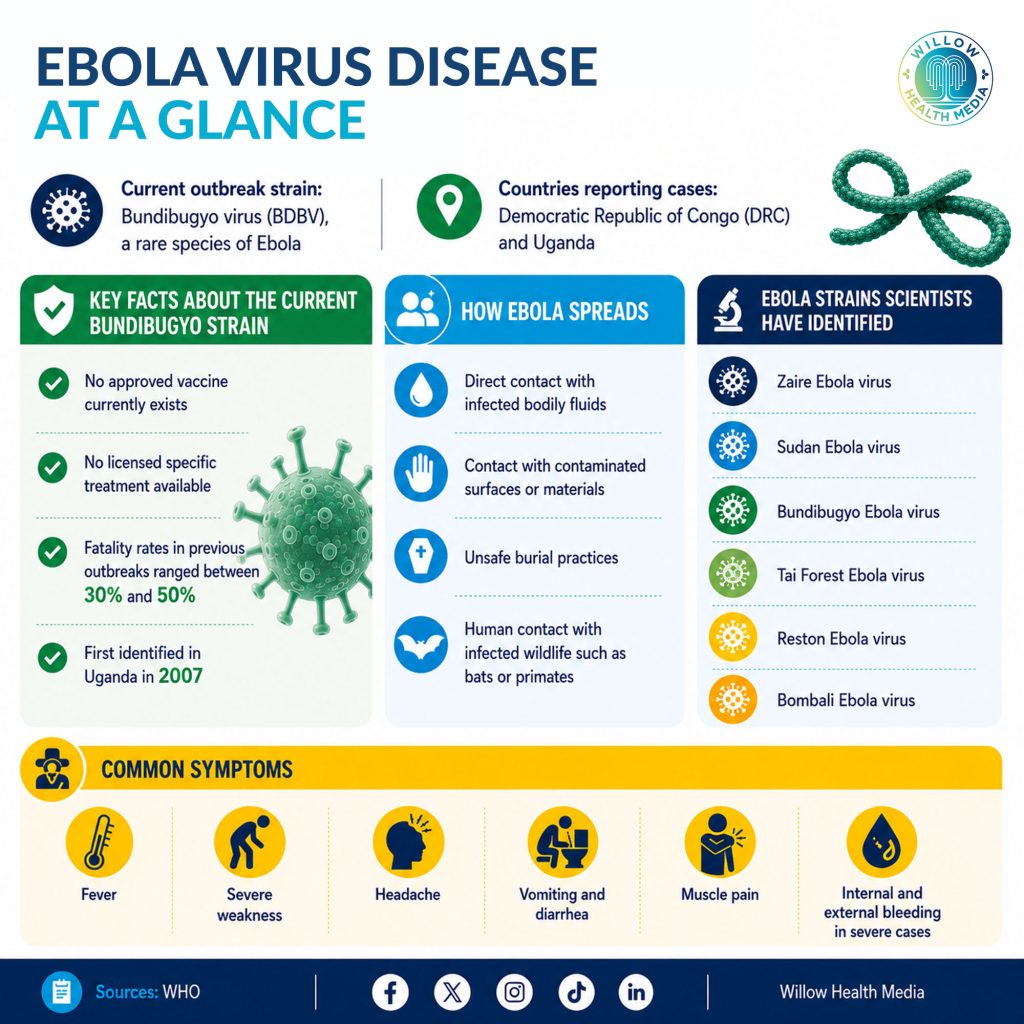
The WHO has described the outbreak as one of the most serious Ebolavirus emergencies in recent years, complicated by insecurity in eastern DRC, limited healthcare access, funding shortages and public mistrust. Unlike the more common Zaire strain, the Bundibugyo variant lacks approved vaccines such as Ervebo, making containment heavily reliant on rapid testing, isolation, contact tracing and supportive care.
The High Court ruling places the Kenya-US arrangement on hold as debate intensifies over the country’s role in international outbreak response, and broader questions over sovereignty, transparency and healthcare capacity remain unresolved.















