
Unlike diseases that remain geographically contained, Ebola travels with people. A trader crossing a border, a family member visiting relatives or a transit passenger can unknowingly create a new chain of transmission. Just why East African region is racing to build the systems that can stop it at the border and within communities.
As the Bundibugyo Ebola outbreak in the Democratic Republic of Congo (DRC) and Uganda continues to expand, East African nations are intensifying preparedness measures to prevent cross-border transmission. With no approved vaccine or specific treatment for this strain, the response depends on early detection, community surveillance and cross-border coordination. While the region has made significant progress, the World Health Organization (WHO) warns that gaps remain and that outbreaks can arrive from unexpected directions.
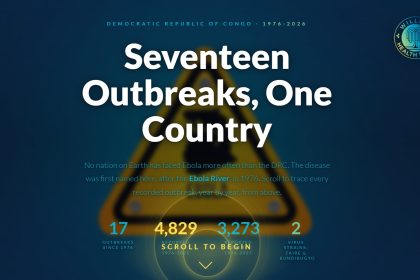
The Ebola virus is among the world’s most feared infectious diseases: highly lethal, fast-moving and capable of exploiting any gap in public health systems. The current outbreak, caused by the Bundibugyo strain, was declared a Public Health Emergency of International Concern in May 2026, with its epicentre in DRC’s Ituri Province and confirmed cases in Uganda’s capital, Kampala.

For Dr Allan Mpairwe, Technical Officer for Risk Management and Emergency Preparedness at the World Health Organization (WHO), the threat demands more than reactive measures. “Preparedness is a process. It is a journey,” he says. “It begins with understanding your risks and planning for them effectively.”
WHO has classified the risk in DRC as very high, while countries sharing land borders with DRC and Uganda face a high risk. The reasons are structural. “We have porous borders, trade corridors, people moving between countries and strong family ties across border communities,” Dr Mpairwe explains. “There is often a very thin line between one country and another.”
Unlike diseases that remain geographically contained, Ebola travels with people. A trader crossing a border, a family member visiting relatives or a traveller transiting through a transport hub can unknowingly seed a new chain of transmission. This reality means countries across East Africa must maintain vigilance even when outbreaks are occurring outside their borders.
Communities are often the first to detect unusual illnesses, unexplained deaths, changes in health patterns
One of the clearest lessons from both Ebola outbreaks and the COVID-19 pandemic is that disease control begins within communities. “At WHO, we put the community at the centre of preparedness because outbreaks begin and end in the community,” says Dr Mpairwe.
Historically, outbreak responses concentrated on hospitals, laboratories and emergency response teams. While these remain essential, public health experts now recognise that communities are often the first to detect unusual illnesses, unexplained deaths or changes in health patterns. “The communities should own surveillance and be part of the process,” Dr Mpairwe says.

Community ownership matters because public health interventions are far more effective when local populations trust and actively participate in them. Without that trust, misinformation spreads, people avoid health facilities, and contact tracing breaks down. To build it, WHO and national governments work closely with religious leaders, opinion leaders and respected community members. “We work with them, not for them,” Dr Mpairwe says. “For as long as we do not build trust, it becomes very difficult to ensure preparedness is rolled out.”
Survivors of previous outbreaks are also being drawn into preparedness efforts. Their accounts help communities understand disease risk while reinforcing confidence in public health interventions.
At the centre of community-based surveillance are community health workers. These frontline workers live in the same communities they serve, making them uniquely placed to detect unusual health events before they escalate. “Community health workers are among the first people to identify unusual diseases or unusual deaths in the community,” Dr Mpairwe says.
COVID-19 pandemic accelerated surveillance, laboratory networks and emergency response structures
Their work extends beyond detection. They report suspicious cases to health facilities, educate residents, mobilise communities during emergencies and disseminate critical health information. In Ebola preparedness, they also help facilitate safe burial practices, one of the key transmission risks in any outbreak. “Engaging community members from within that community helps build trust and ensures people believe in what responders are saying,” Dr Mpairwe explains.
The COVID-19 pandemic transformed health systems across the world. Though it stretched resources to their limits, it also accelerated investment in surveillance, laboratory networks and emergency response structures. For Dr Mpairwe, the central lesson is clear. “Early detection and response are very important. For as long as you identify diseases as early as possible, you are able to contain them.”

Countries that built preparedness systems before crises hit consistently achieved better outcomes. Critical investments include community-based and border surveillance, laboratory capacity, Emergency Operations Centres, rapid response teams, risk communication mechanisms, health workforce training and community engagement programmes.
To support at-risk countries, WHO has developed preparedness packages guiding governments on essential actions before outbreaks occur. For priority countries such as Kenya, which share proximity with affected regions and are connected through key transport corridors, these efforts are being intensified. Governments are training clinicians, surveillance officers and contact tracing teams, while simulation exercises test whether systems function under realistic outbreak scenarios. “You need to test your systems,” Dr Mpairwe says. “That is why we are doing a lot of simulation exercises.”
Kenya’s public health preparedness has improved significantly in recent years. Community-based surveillance has expanded, health facility surveillance has strengthened, and laboratory capacity has grown substantially, enabling faster identification and investigation of suspected cases. “There has been great improvement in surveillance systems, particularly here in Kenya,” Dr Mpairwe says. “The investments during COVID have played a key role in responding to the current threat.”
Establishing advanced laboratory capacity in every county is costly and often impractical
The country is also assessing treatment facilities, training healthcare workers and strengthening emergency response structures. “The Ministry of Health and the National Public Health Institute are leading a lot of work, and I think they are on track,” Dr Mpairwe says.
Despite the progress, gaps remain. Establishing advanced laboratory capacity in every county is costly and often impractical. “You may not possibly close all the gaps, but at least you ensure that the gap is not so wide as to prevent responders from doing what they are supposed to do,” Dr Mpairwe says.
Disease outbreaks do not respect political boundaries. Across East Africa, countries routinely exchange information, redefine surveillance zones and strengthen monitoring around border crossings. WHO works alongside regional partners, including the International Organization for Migration (IOM) and the East African Community (EAC), to strengthen cross-border health security systems. “WHO is a technical agency, and our main strength is providing technical support to member states. So, we guide them on what key actions are supposed to be taken to enhance surveillance at borders,” Dr Mpairwe says.
These partnerships help countries implement the International Health Regulations and reduce the risk of diseases spreading across borders.
The most pressing question for many East Africans is whether their countries could respond effectively if Ebola arrived tomorrow. Dr Mpairwe believes important capacities are already in place. Suspected alerts have been investigated and ruled out through laboratory testing, demonstrating that surveillance and diagnostic systems are functioning.
Where borders are porous but cooperation is growing, preparedness is the most powerful tool in preventing the next outbreak
Kenya has identified high-risk counties and is assessing facilities for use as treatment and isolation centres. “We are currently assessing health facilities and potential treatment units for Ebola. So, there is a lot that is going on,” Dr Mpairwe says.

He cautions, however, that outbreaks are unpredictable. “We may be focusing on the borders, and then it comes from the community.” Preparedness is therefore not about predicting precisely where the next outbreak will begin. It is about ensuring systems can respond effectively regardless of where it does.
The ultimate goal extends beyond the current Ebola threat. Strong surveillance systems, trained health workers, resilient laboratories and engaged communities improve responses to every public health emergency, whether Ebola, Marburg or a future unknown pathogen. “It is about investing in community knowledge, investing in skills, investing in workforce development and working together as a community,” Dr Mpairwe says.
In a region where borders are porous but cooperation is growing stronger, preparedness may prove to be the most powerful tool in preventing the next outbreak from becoming a regional crisis.
This story was first published by Willow Health Media on June 24, 2026.















