

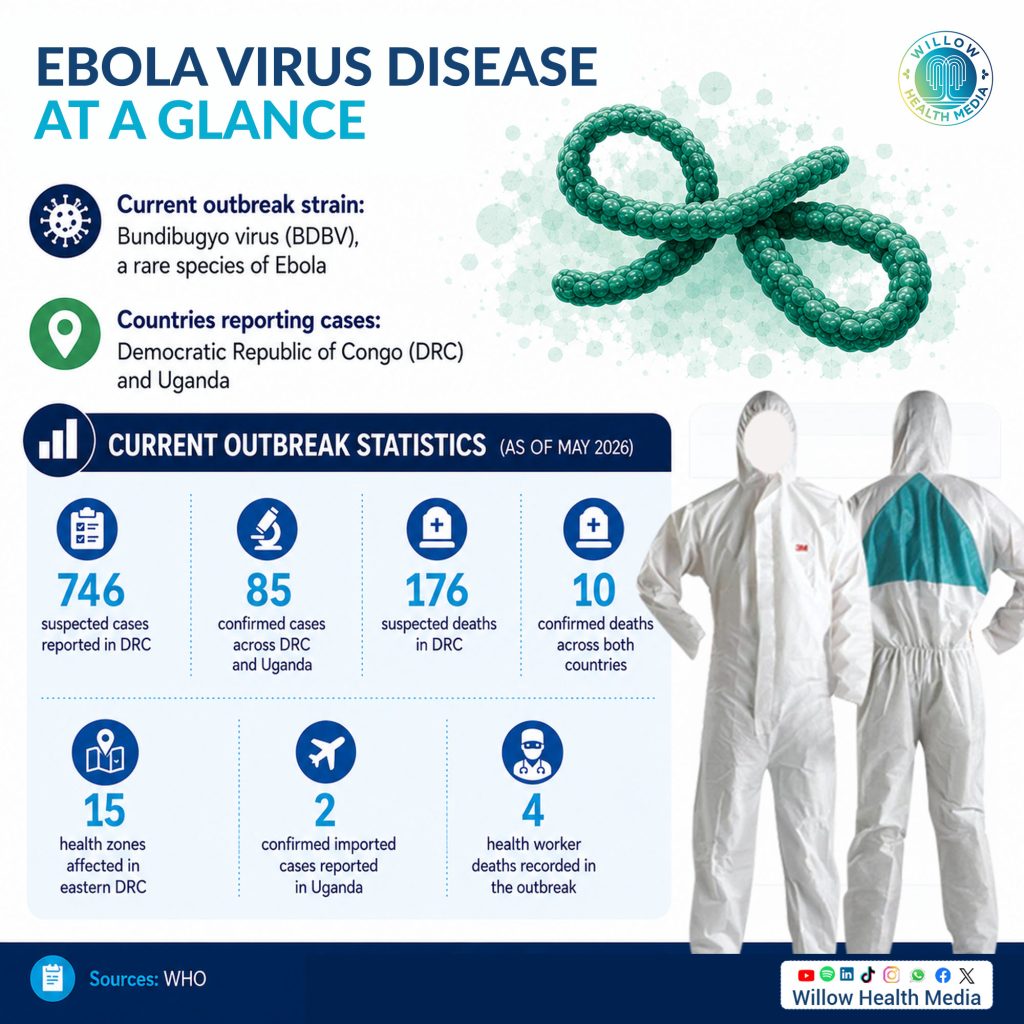
A rare and poorly understood strain of Ebola called Bundibugyo is driving a rapidly worsening outbreak in the Democratic Republic of Congo (DRC) and Uganda, one that has been declared a global health emergency. Unlike the more familiar Zaire strain, Bundibugyo has no approved vaccine or treatment, and it kills between 30 and 50 per cent of those it infects.
Health experts warn that weak health systems, mistrust of authorities, and unsafe burial practices are making containment harder, while early symptoms that mimic malaria or typhoid mean many cases are caught too late.
Why is Bundibugyo Ebola so dangerous?
A disease that looks like malaria at first, kills within days, and has no vaccine. That is the challenge health authorities in Central and East Africa are now confronting as the Bundibugyo strain of Ebola spreads across the DRC and Uganda, placing the world on alert.
The World Health Organisation (WHO) declared the outbreak a Public Health Emergency of International Concern on May 17, 2026. According to WHO, by May 2026, the DRC had reported more than 746 suspected cases and at least 176 suspected deaths, with confirmed cases across both countries surpassing 85.
Dr Moses Masika, an infectious diseases expert, describes Ebola Virus Disease as “one of the most severe viral haemorrhagic fevers known to humanity.”
What is Ebola and where did it come from?
Ebola is caused by a group of viruses belonging to the Filoviridae family. The disease was first identified in 1976 near the Ebola River in what is now the DRC. Since then, Africa has experienced multiple outbreaks, with the deadliest occurring in West Africa between 2014 and 2016, killing more than 11,000 people.
“It attacks multiple organs in the body and weakens the immune system very rapidly, which is why patients can deteriorate within days,” Dr Masika explains.
Fruit bats are believed to be the natural reservoir of the virus, with outbreaks often beginning after human contact with infected wildlife. “The virus can spill over from animals to humans, especially in areas where people interact closely with wildlife through hunting, bushmeat consumption or deforestation activities,” Dr Masika says.
The strains: not all Ebola is the same
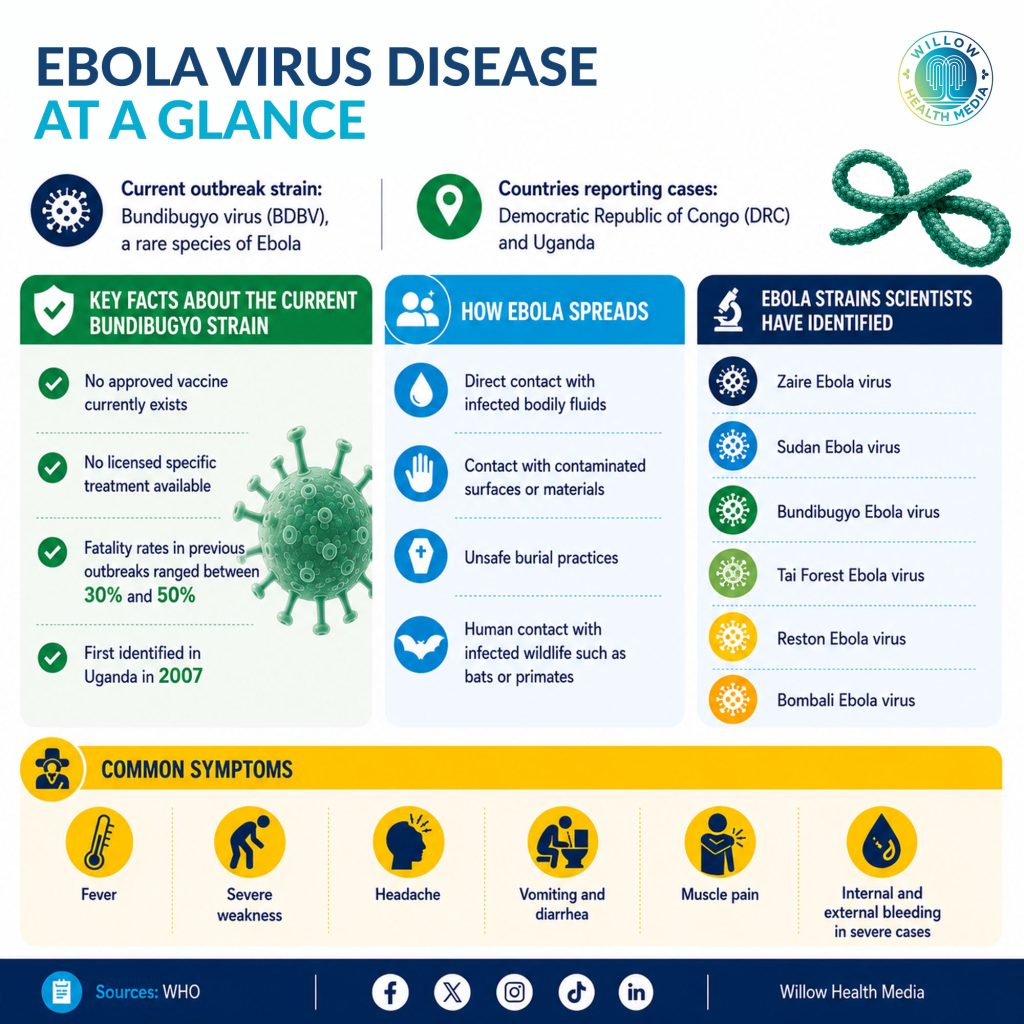
Scientists have identified six known Ebola species: Zaire, Sudan, Bundibugyo, Tai Forest, Reston and Bombali. Three of these – Zaire, Sudan and Bundibugyo – are responsible for most large outbreaks in Africa.
“The Zaire strain is historically the deadliest and was responsible for the West African epidemic. The Sudan strain has also caused serious outbreaks in Uganda. What we are now seeing is the Bundibugyo strain, which is rarer but still extremely dangerous,” Dr Masika explains.
Crucially, the Bundibugyo strain is different enough from Zaire that existing Ebola vaccines – which were developed against the Zaire strain – offer limited or no protection against it. There is no licensed vaccine or specific treatment approved for Bundibugyo. Previous outbreaks of the strain recorded fatality rates ranging from 30 to 50 per cent.
“This is what makes the current outbreak worrying. We are dealing with a strain that is less studied, has no approved vaccine and emerged in areas facing insecurity and weak health systems,” Dr Masika says.
The current outbreak is additionally complicated by the fact that many field laboratories were configured to detect the Zaire strain, meaning Bundibugyo infections circulated undetected for weeks before the outbreak was confirmed.
How does it spread?
Ebola is highly infectious, but it is not airborne. It spreads through direct contact with bodily fluids – including blood, saliva, sweat, vomit, urine and semen – or contaminated surfaces. Unlike COVID-19, transmission requires close physical contact with an infected person or contaminated materials.
Unsafe burial practices have historically played a major role in accelerating Ebola outbreaks because the bodies of those who die from the disease remain highly infectious long after death.
“In many outbreaks, fear becomes almost as dangerous as the virus itself. Some communities hide patients, resist isolation or conduct unsafe burials, which accelerates spread,” Dr Masika warns.
Symptoms: Why early diagnosis is so difficult
Ebola symptoms appear between two and 21 days after infection. The early signs closely resemble many common tropical illnesses, making diagnosis difficult in the critical early window.

Patients initially develop fever, fatigue, headache, muscle pain, sore throat and weakness before progressing to vomiting, diarrhoea, internal bleeding, organ failure and shock.
“Many people think bleeding is always the first sign of Ebola, but that is incorrect,” Dr Masika says. “Most patients first experience symptoms that look like malaria, typhoid or influenza. By the time bleeding occurs, the disease is already severe.”
At a physiological level, “the virus essentially overwhelms the body’s immune defences and destroys the integrity of blood vessels, leading to fluid loss, shock and in severe cases, death,” he explains.
Will Ebola spread globally?
Despite the scale of the current outbreak, experts say Ebola is unlikely to spread globally the way COVID-19 did.
“Ebola requires close physical contact for transmission, which makes it easier to contain compared to respiratory viruses,” Dr Masika explains. “However, urban outbreaks and cross-border movements still pose serious regional risks.”
WHO currently considers the risk of wider international spread moderate, particularly in countries connected to the DRC and Uganda through trade and migration routes.
Treatment and the best available defences
There is currently no universally approved cure for all Ebola strains. For Bundibugyo specifically, treatment is limited to supportive care: intravenous fluids, oxygen therapy, blood pressure management and treatment of secondary infections.
“The earlier patients are isolated and given supportive care, the better their chances of survival,” Dr Masika says.

Public health measures remain the strongest tools available: rapid testing, patient isolation, contact tracing, hand hygiene, safe burials and community awareness campaigns.
“Ebola is not just a medical problem; it is also a community problem. Outbreaks are controlled when people trust health workers, report symptoms early, and follow prevention guidelines,” Dr Masika says.
Scientists are working to develop vaccines and treatments specifically targeting the Bundibugyo strain. Until those are available, health officials say vigilance, early detection and community cooperation remain the most effective defences against one of the deadliest viruses known to medicine.















