

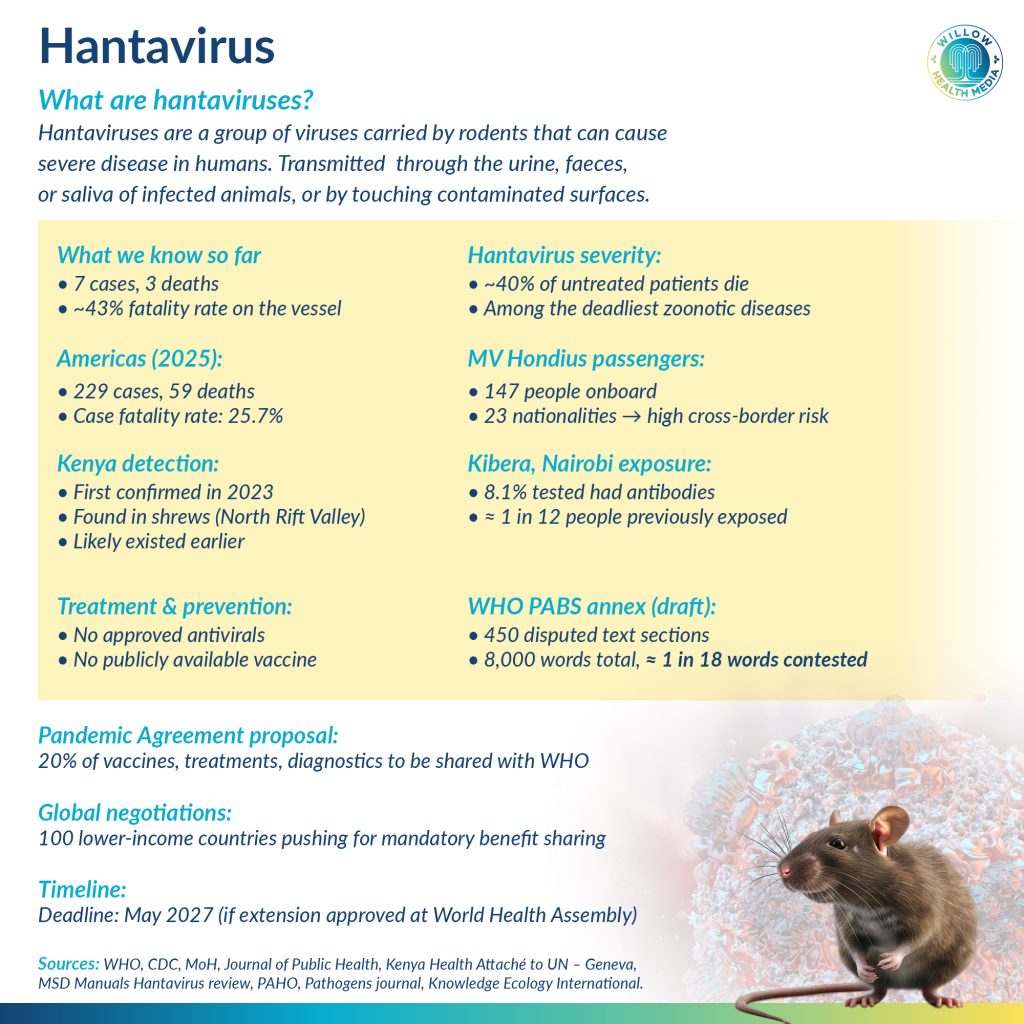
A cruise ship carrying 147 people from 23 countries has just reported three deaths from a virus with no cure. A 2023 study in Nairobi’s Kibra area found that 8.1 per cent of people tested had hantavirus antibodies, pointing to quiet but real circulation of the virus in dense urban communities.
A Dutch cruise ship travelling through the remote South Atlantic reported a deadly hantavirus outbreak in late April 2026, killing three of its 147 passengers and crew. The disease has no approved treatment or vaccine. It arrived days after negotiations on a critical World Health Organisation (WHO) Pandemic Treaty provision, designed to ensure poorer countries benefit fairly from pathogens they share with the world, collapsed in Geneva. For Kenya, a country with its own hantavirus exposure and a prominent seat at those negotiations, the timing was impossible to ignore.

Hantavirus is a rodent-borne disease. People catch it through contact with the urine, faeces, or saliva of infected animals, or by touching contaminated surfaces. It does not ordinarily pass between people. The exception is the Andes virus, found in Chile and Argentina, which is the only known strain capable of spreading from person to person and the suspected strain in the current hantavirus outbreak.
The disease starts with fever, chills, muscle aches and headache, then moves rapidly to fluid in the lungs, low blood pressure, and irregular heart rhythms. Without treatment, it kills up to 40 per cent of those infected. In 2025 alone, eight countries in the Americas reported 229 cases and 59 deaths, a fatality rate of 25.7 per cent.
The ill-fated ship, MV Hondius, operated by Dutch tour company Oceanwide Expeditions, left Ushuaia, Argentina, on April 1 and travelled through some of the most remote waters in the world, including Antarctica, South Georgia, Tristan da Cunha, and Saint Helena. According to WHO’s Disease Outbreak News published on May 4, seven cases were identified among passengers and crew from 23 nationalities, two confirmed and five suspected. Three people have died.
Some people on the ship were couples sharing rooms, so that’s quite intimate contact
The situation worsened. At a press briefing on May 5, WHO technical adviser Maria Van Kerkhove said person-to-person transmission could no longer be ruled out. “We do believe there may be some human-to-human transmission happening among very close contacts. Some people on the ship were couples; they were sharing rooms, so that’s quite intimate contact,” she said.

Three symptomatic passengers were evacuated to shore. Spain agreed to receive the vessel at a port in the Canary Islands after Cabo Verde refused it entry. Laboratory confirmation was conducted by South Africa’s National Institute for Communicable Diseases, with further samples sent to the Institut Pasteur de Dakar in Senegal for genome sequencing.
Hantavirus rarely comes up in Kenya’s public health discussions. The evidence suggests it should.
A 2023 study in the journal Pathogens reported the first detection of hantavirus in Somali shrews trapped in Kenya’s North Rift Valley, finding that farming and shelter construction increase rodent contact and the risk of the disease crossing into human populations. A separate study in Kibra, Nairobi’s largest informal settlement, found that 8.1 per cent of people tested had hantavirus antibodies, pointing to quiet but real circulation of the virus in dense urban communities.
Kenya’s farming communities in the Rift Valley live in conditions that match the textbook risk profile: shared spaces with rodents, disturbed soil, stored grain, and limited access to protective equipment or quick diagnostic tools. The country’s Zoonotic Disease Unit, established in 2011, coordinates responses to Rift Valley fever, anthrax, and brucellosis. Hantavirus has not made that priority list, despite the evidence.
In 2025, the World Health Assembly adopted the WHO Pandemic Agreement with Kenya as one vocal champion
The outbreak landed differently in Geneva, where Kenya’s diplomats had just emerged from a week of failed treaty negotiations. “The emergence of the hantavirus outbreak feels like an uncomfortable reminder to all of us,” said Dr Jean Gitau, Kenya’s Health Attaché to the United Nations in Geneva. “It raises that unfamiliar discomfort we all felt during COVID. Here, people are confined to a cruise ship, and they cannot move.”
In May 2025, the World Health Assembly adopted the WHO Pandemic Agreement, a global legal framework designed to prevent a repeat of the inequities that defined the COVID-19 response. Kenya was one of its most vocal champions. Health Cabinet Secretary Aden Duale pushed at the assembly for the rapid completion of the Pathogen Access and Benefit Sharing annex, known as PABS, calling it essential to a fair global health system. He specifically sought technology transfer provisions that would allow Kenya to gain something tangible from the pathogens it shares with international researchers.
The argument is grounded in what happened during COVID-19. African countries, including Kenya, shared genetic sequencing data on new variants quickly, helping scientists globally develop vaccines faster than ever before. The vaccines came back late, in small quantities, and at prices that stretched public health budgets.
The Pandemic Agreement would require pharmaceutical manufacturers to make up to 20 per cent of their vaccine, treatment, and diagnostic production available to the WHO during a pandemic emergency. That single provision, if enforced, would fundamentally change what Kenya receives the next time a new pathogen emerges.
Dr Gitau frames the stakes directly. “The global north has all the manufacturing capacity, the technology, the money, and the ability to develop vaccines, treatments, and diagnostics. When we don’t see any benefits, where is the motivation to share pathogens? In the absence of this PABS system, those questions remain unanswered.”
Wealthier nations have resisted, prioritising protection of pharmaceutical industry interests
The sixth and final scheduled round of negotiations ended on May 1 without a completed PABS annex. A seventh session has been scheduled for July 6 to 17, with the outcome going before the 79th World Health Assembly opening May 18. Member states will be asked to extend negotiations through to May 2027.

The gap between the two sides is not subtle. At the April 30 session, Knowledge Ecology International noted that the latest draft contained 450 sets of brackets marking unresolved text in a document of nearly 8,000 words.
Around 100 lower-income countries have demanded mandatory benefit sharing as the condition for sharing pathogen data. Wealthier nations have resisted, prioritising protection of pharmaceutical industry interests and open access to genetic sequence data. Neither side has moved enough.
Dr Gitau is worn down but not without hope. “Session by session, the gap proved to be stubborn and growing bigger. Core disagreements remained unresolved. We are hoping that over the next few months, we are able to find a solution so that the discoordination during COVID is not repeated.”
For Kenya, the ship is also a mirror as it has rodents, dense informal settlements and farming communities
The MV Hondius is heading to Spain. Its samples are being processed in South Africa and Senegal. Its data will move through laboratories across the world. That chain of international cooperation, working under pressure in the middle of an ocean, is precisely what the pandemic treaty is meant to protect and formalise.

For Kenya, the ship is also a mirror. It has the rodent populations, the dense informal settlements, the farming communities, and the data-sharing record that make this outbreak both a biological and political concern. What it does not yet have is a guarantee that what it contributes to global health will be matched by equal protection when the next outbreak arrives.
“Even if this virus does not spread easily from person to person,” Dr Gitau said, “who shares information quickly? Those people sharing information, what benefits will they receive? In the event that hantavirus spreads to their population, what do they get? In the absence of this PABS system, those questions remain unanswered.”















