More than 18,000 people potentially exposed to Ebola in eastern DRC are unaccounted for and unmonitored. Africa CDC warns that every missing contact is a transmission chain that nobody can see, trace or stop.
Red dust hangs low over the mining fields of Mungwalu in eastern Democratic Republic of Congo as young men emerge from shafts carved deep into the earth. Their work connects them to a vast network of traders, transporters, relatives and fellow miners moving daily between villages, markets and border towns.
But among them could be someone exposed to Ebola. Not a confirmed patient or someone in isolation, but a contact. Someone who shared a meal with an infected relative, cared for a sick friend, or attended a hurried burial. If that person remains unidentified and unmonitored, they become part of an invisible chain of transmission capable of carrying the virus far beyond the mining town where the outbreak began.
That invisible chain is now one of the greatest concerns for health officials responding to what the Africa Centres for Disease Control and Prevention (Africa CDC) describes as the third-largest Ebola outbreak on the continent since the virus was first identified.
While headlines focus on confirmed cases and deaths, Africa CDC says a more troubling figure is emerging behind the scenes: thousands of people who should be under surveillance are missing from the response altogether.
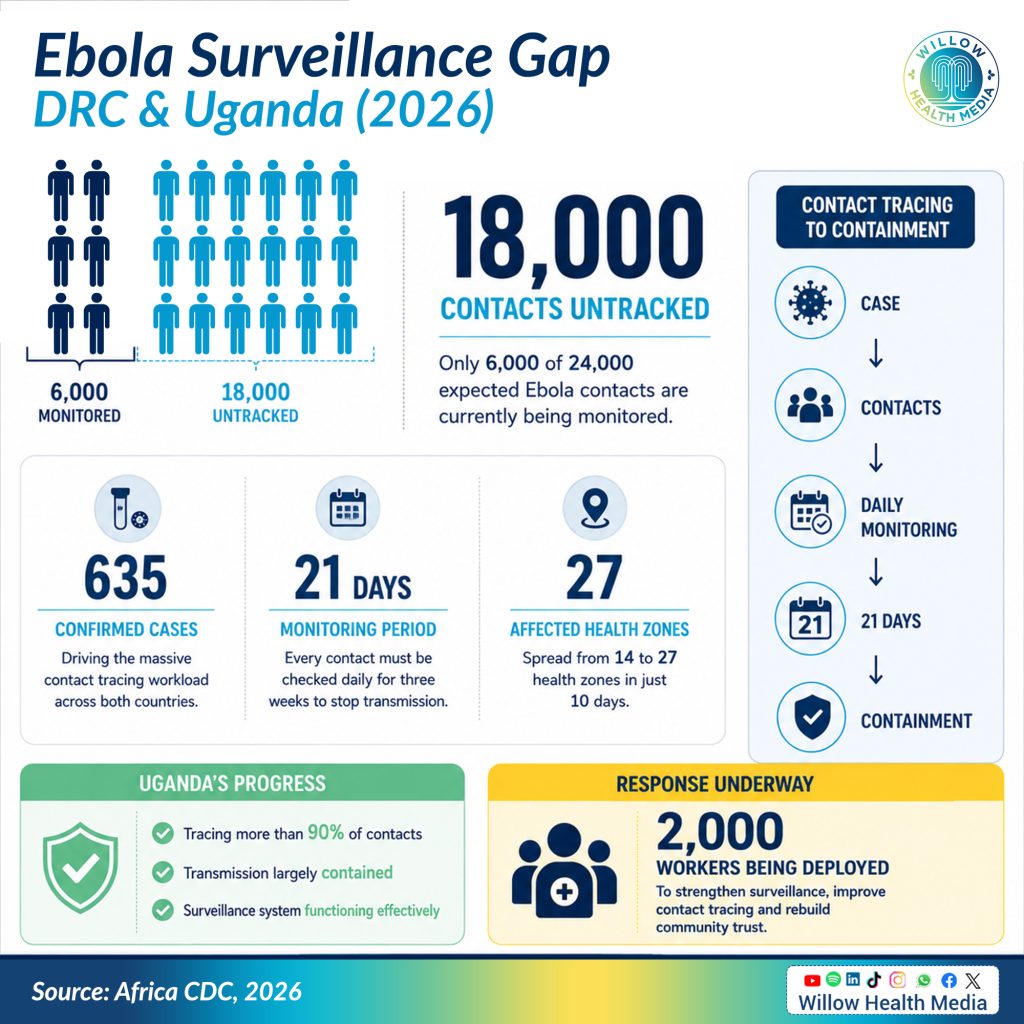
For approximately 635 confirmed Ebola cases reported across the Democratic Republic of Congo (DRC) and Uganda, health officials would ordinarily expect around 24,000 contacts to be identified and monitored. Instead, only about 6,000 people have been listed as contacts, and only a portion of those are being actively followed.
The gap means that more than 18,000 potentially exposed individuals may not be under any form of routine monitoring.
“If we don’t know these people, if we don’t have them on the list, if we don’t follow up, it means there is a huge risk of transmission being sustained in the community,” Africa CDC Director General Dr Jean Kaseya warned during a briefing on June 11.
Once a case is confirmed, health workers identify everyone the infected person interacted with
For outbreak responders, this is not a mere statistical shortfall. It is the difference between containing a virus and allowing it to spread unnoticed through communities.
For diseases like Ebola, contact tracing remains one of the most effective tools available. The process is straightforward in principle. Once a case is confirmed, health workers identify everyone the infected person interacted with before symptoms appeared. Those contacts are then monitored daily for 21 days, checked for symptoms and rapidly isolated if they fall ill. When done effectively, contact tracing breaks chains of transmission before they expand into larger outbreaks.
In eastern DRC, however, the system is struggling under extraordinary pressure. The outbreak is concentrated in areas affected by insecurity, population displacement and extensive mining activity. The number of health zones affected by Ebola doubled from 14 to 27 within just ten days, according to Africa CDC data. Armed conflict, attacks on health facilities, community mistrust and logistical barriers are all hampering the ability to reach remote communities consistently. In some areas, insecurity has forced humanitarian flights to stop operating. Treatment centres have been attacked or damaged. “We still have a lot to do, a lot,” Dr Kaseya acknowledged.
Many of those most affected are young adults between the ages of 15 and 44, the same demographic that dominates mining, transport and cross-border trade. “We really need to target the youth. If we don’t target this group, we will not stop this outbreak,” Dr Kaseya said.
Without an approved vaccine or treatment specifically designed for the Bundibugyo species driving the current outbreak, public health officials say they must return to what they call the fundamentals of outbreak control. Central to that strategy is the deployment and rapid training of approximately 2,000 community health workers across affected areas.
They explain symptoms, counter misinformation, identify suspected cases, encourage testing
“We don’t have vaccines and therapeutics for the current Bundibugyo virus. So we need to return to the basics of epidemiology,” said Dr Wissam Mankoula, an Africa CDC outbreak specialist.
Rather than relying solely on centrally deployed response teams, the approach seeks to empower trusted local figures who understand the terrain, speak local languages and have established relationships within communities. These workers do more than collect health data. They explain symptoms, counter misinformation, identify suspected cases, encourage testing and help families understand why contact tracing matters.

“We need to have those 2,000 community workers on the ground, engaging the community, making sure that they are part of the solution,” said Professor Yap Boum, Deputy Incident Manager supporting the response.
Early signs suggest the strategy is working. Professor Boum noted that some patients are now presenting themselves voluntarily at treatment centres after hearing information on the radio or learning that relatives had shown symptoms. Each self-referral represents a potential transmission chain interrupted before it expands. Rather than treating communities as passive recipients of health messages, the response increasingly views them as active participants in outbreak control. As Dr Kaseya put it: “We cannot provide solutions without themselves.”
The emphasis on community-based surveillance is not new to Kenya. Across the country, Community Health Promoters (CHPs) have become one of the most visible pillars of primary healthcare. Working at the household level, they provide health education, monitor vulnerable families, identify early signs of disease outbreaks and connect communities with formal health services. Their role became particularly visible during the Covid-19 pandemic, when they helped identify suspected cases, educate communities and counter misinformation.
When outbreaks occur, the first warning signs emerge from communities long before they appear in hospitals or labs
Kenya’s community health strategy has gained increased attention as the government expanded support for CHPs as part of broader Universal Health Coverage reforms. Public health specialists have long argued that such community-based systems are not simply healthcare delivery mechanisms. They are also essential components of epidemic preparedness. When outbreaks occur, the first warning signs often emerge at the community level long before they appear in hospitals or laboratories.
Uganda offers a glimpse of what effective contact tracing can achieve. According to the Africa CDC, Uganda has identified nearly all expected contacts linked to its Ebola cases, with more than 90 per cent under active daily follow-up. New infections are emerging primarily from known contact networks rather than unexplained community transmission. “I can say the outbreak is really under control in Uganda,” Dr Kaseya said.
Africa CDC officials have pointed specifically to Uganda’s strong contact tracing performance as the key driver of that outcome. When health authorities know where transmission is occurring, they can intervene quickly. When infections emerge from unknown sources, the outbreak becomes significantly harder to contain.
Big lesson from DRC is that epidemic response begins long before a patient arrives at a border crossing
Although the outbreak remains concentrated in DRC and Uganda, health security experts stress that infectious diseases do not respect national borders. Eastern Africa’s transport corridors connect mining towns, border posts, cities and international airports through the constant movement of people and goods.

Recognising this, Africa CDC has begun promoting harmonised health screening systems across the continent, including QR-code-based verification mechanisms intended to improve information sharing between countries.
The deeper lesson emerging from eastern DRC is that epidemic response begins long before a patient arrives at a border crossing. It begins with trusted individuals embedded within communities, people capable of identifying unusual illnesses, encouraging early care-seeking and helping public health authorities understand where disease may be spreading.
The missing 18,000 contacts represent more than a surveillance challenge. They represent a test of whether health systems can reach communities quickly enough, build trust deeply enough and act decisively enough to interrupt transmission. The solution is neither new nor complex. It relies on local knowledge, trusted relationships and frontline workers willing to knock on doors, answer questions and guide families through uncertainty.
Whether in the mining settlements of Mungwalu, the villages of Ituri or communities across Kenya, the principle remains the same. As Professor Boum reminded reporters: “Everything starts and ends with the community.”