

She used to spend her days in delivery rooms, catching babies. Now she spends them in labs, chasing a bacterium. The shift cost her a comfortable routine, but it may save thousands of lives.
In our latest episode of Whitecoat Diaries, Dr Koech opens up to Willow Health Media Editor-in-Chief, DR MERCY KORIR, on how one question from a woman in Kilifi shifted her from clinical practice to research.
There is a question a woman once asked Dr Angela Koech at a community meeting in Kilifi, and it has stayed with her ever since.
Dr Koech is a Research Physician Scientist and an Assistant Professor of Obstetrics and Gynaecology at Aga Khan University. She recalled explaining to the women about the importance of antenatal clinics when one woman asked, “But there is a woman in my village who came for antenatal care. She came for all her visits. She did everything she was told, and she still lost that baby. Why?”
In her mind’s eye, Dr Koech can still see the woman asking that question. It made her ask herself: “How can you tell women to come to antenatal care if you cannot promise them, or at least give them hope, that they will prevent some of these conditions?”
This is why Dr Koech, the co-principal investigator of the PRECISE Project at the Centre of Excellence in Women and Child Health, has devoted her career to stopping the losses before they happen.
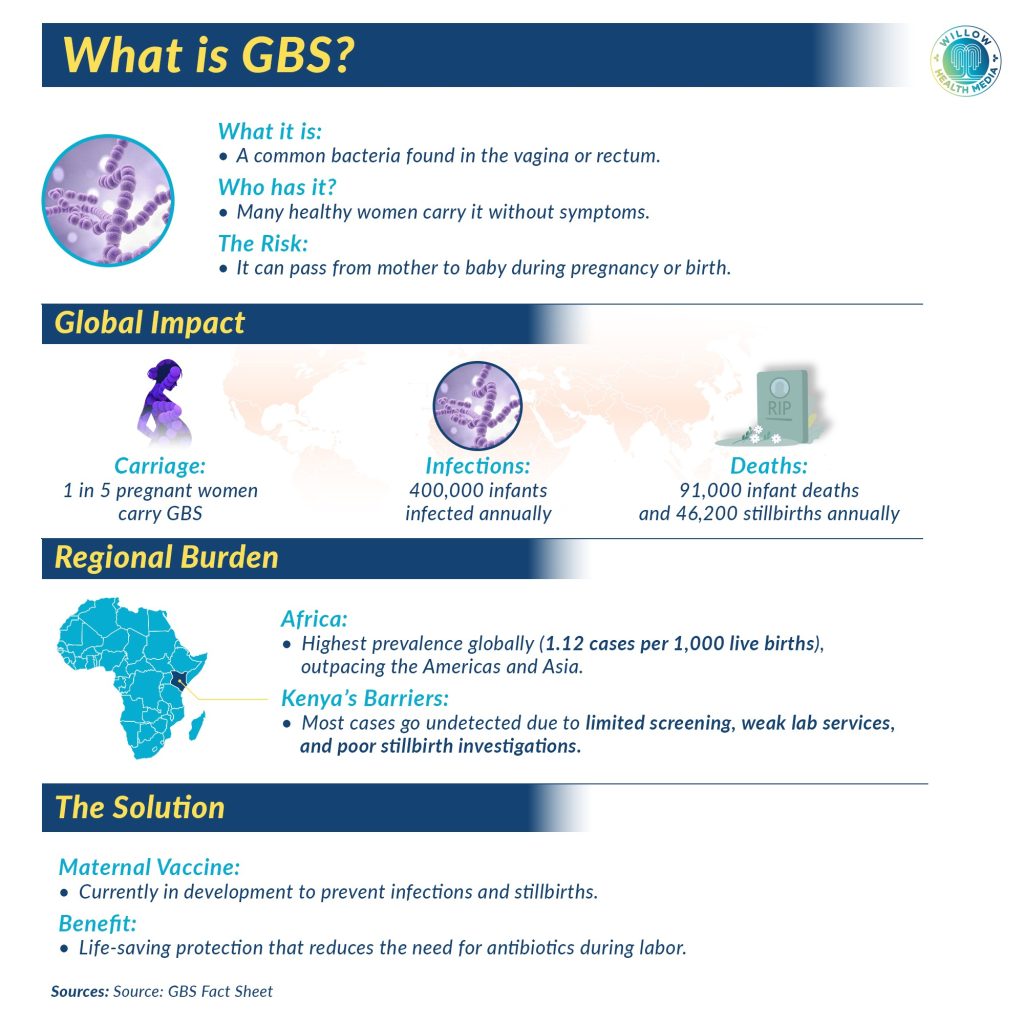
Right now, her focus is on a bacterium that most Kenyans, and many clinicians, have never heard of: Group B Streptococcus (GBS). This is a silent, common and entirely asymptomatic bacterium in mothers who carry it. For the babies it infects, it can be lethal within hours.
GBS spreads from mother to baby during birth without either being aware
GBS has been known to cause serious infections in newborns for decades. What makes it particularly dangerous in Kenya and sub-Saharan Africa is a combination of factors. It cannot be detected without a specific test that most facilities cannot perform. It spreads from mother to baby during birth without either being aware. And by the time the sick baby reaches a hospital equipped to treat it, it is often too late.
Dr Koech explains the transmission simply: “Most of the time, it is obtained from the mother’s reproductive tract. In late pregnancy and during birth, the bacteria transfers from the mother to the baby. It may just sit on the baby’s body. That is fine. But occasionally it may enter the respiratory tract. In that case, it gives the baby invasive disease, meaning the bacteria is now in the baby’s circulation. The baby would have sepsis, and sometimes it could even enter the nervous system and give the baby meningitis.”
Worldwide, there are an estimated 394,000 cases of invasive GBS disease in early infancy each year, with approximately 58,300 deaths. Sub-Saharan Africa carries the heaviest burden, accounting for around 90,800 early-onset cases, mostly in countries where the infrastructure to diagnose and treat the infection is most limited.
In sub-Saharan Africa, almost one in four newborns with early-onset GBS disease will die from it. One in ten survivors will live with moderate or severe neurodevelopmental impairment. Kenya already records a neonatal mortality rate of 21 deaths per 1,000 live births, about 92 newborns every day. GBS is not responsible for all of those deaths, but its contribution is almost certainly undercounted.
The particular cruelty of GBS is that the carrier, the mother, has no idea.
“In most mothers, it is an asymptomatic infection. The mother is simply a carrier. The bacteria sit in the reproductive tract. The mother is absolutely fine without symptoms or signs of illness or fever. This would be a healthy pregnant mother who gives birth in the normal way,” Dr Koech explained.
The pregnant women were healthy, symptom-free…but carried GBS
In research conducted in Kilifi County, Dr Koech and her team found that about 11 per cent of women who came in to deliver were carrying GBS. At one site, the figure reached 14 per cent. These women were healthy, symptom-free and not expecting any problems.

In context: if a busy county maternity unit delivers 500 women a month, more than 50 of those mothers may unknowingly carry a bacterium capable of making their babies critically ill.
The only way to know is to test. But a GBS swab requires a culture, a process that takes one to three days, demands laboratory equipment available only at certain Level Four and Level Five hospitals, and requires a chain of record-keeping that can track a woman from her antenatal visit through to labour. In a public health system stretched across a vast geography, that chain breaks constantly.
“Even basic and simple tests that women need in an antenatal clinic, not all of them get them. We know women need an HIV test, a syphilis test and a test for anaemia. We are talking the very basics. And not all women get these. So first, we all need to improve diagnostics for women overall, before we even address this additional knowledge from Group B Strep,” said Dr Koech.
To explain why a GBS vaccine would be so significant, Dr Koech uses an example that every Kenyan parent knows: the tetanus jab during pregnancy.
A newborn was admitted with convulsions, unable to feed, heavily sedated, but didn’t win
“Many mothers do not realise that the tetanus injection is mostly for the baby. Adults can handle the tetanus infection better. But if a neonate gets tetanus, it is very serious. Many babies die.”
She recalls a baby she cared for during her internship at Kericho District Hospital, a newborn admitted with convulsions, unable to feed, heavily sedated throughout a three-week fight for life that the baby did not win. “To think that that could have been prevented by an injection in a mother’s arm and a few hours of pain. It was very disturbing.”

Two GBS vaccines are currently in clinical development. One is in Phase Three trials, with Kenyan sites participating. Dr Koech speaks about them with measured optimism.
“With all the challenges I have described, no labs to test, challenges in tracking a patient through the healthcare system, I cannot imagine something more effective at preventing GBS infection on a large scale. The beauty of a vaccine is that you can give it to many to protect the few who would have had the infection, without the harm of giving antibiotics to many.”
The GBS vaccine would be given in the third trimester, around 30 to 32 weeks of pregnancy, close enough to birth for maternal antibodies to transfer effectively to the baby, but far enough in advance for the immune system to respond fully. It would require no laboratory, no swab, no culture and no wait.
The tetanus jab was falsely alleged to cause infertility, with politicians amplifying the claims
In a country where only one or two laboratories in an entire county’s public health system can reliably perform bacterial cultures, this matters enormously. The vaccine does not require that infrastructure. That is exactly why Dr Koech calls it “our one opportunity, especially coming from this part of the world.”

Any discussion of a new maternal vaccine must reckon with hesitancy. In Kenya, the tetanus vaccine faced a damaging period of misinformation, falsely alleged to cause infertility, with political figures amplifying the claims. The damage to public trust was real. “When a woman is pregnant, rightfully so, it is a bigger decision for her to make, because she is making it for herself and for her child.”
Beyond GBS, Dr Koech envisions a more intelligent, personalised assessment beginning the moment a woman walks in for her first visit. “I feel that at that first moment we need to know a woman’s risk, by listening to her, listening to her story. That cannot be replaced by any device.”
Asked whether her work has fulfilled what she imagined, the girl who read a novel about fertility treatment in high school and decided she would become a specialist, Dr Koech reflected: “Does it tick the box? Yes. I meet women, and I watch lives being transformed. But the beauty of what I do now is that I also meet women that I wouldn’t have otherwise met. Something that I studied about a certain lab test could be used on a woman five years from today, in a place I would never have gone. And it would change her pregnancy outcome in a small or a big way.”















