

Overstretched health facilities force risky referrals, leaving mothers and newborns exposed, according to the Quality-of-Care Health Facility Assessment report.
Josphine Barasa, a community health promoter (CHP) at Kangemi Health Centre in Westlands Constituency in Nairobi County, says she regularly refers patients to other facilities because essential reproductive and child health services are missing, exposing women, newborns, and adolescents to danger.
“We normally refer them to other facilities,” she said. “A woman who needed scanning services came here. We did not have a scanning machine, so I had to tell her to go to Westlands Health Centre.”
Barasa recalls a woman who didn’t have money for transport, as her husband had only left her with money for food. Poverty, says Barasa, often shows among “residents who could not afford services from nearby private facilities.”

Barasa also recalled a 16-year-old girl who came for abortion services as she wasn’t ready to be a mother.
The teen opted for a secret abortion as there was no privacy at Kangemi Health Centre, as “The hospital does not have an isolated area where an adolescent can have a private session with a professional on any service ranging from reproductive services to maternal and contraceptive services,” explained Barasa.
“With enclosed stations, patients can have private consultations with professionals, like they do in private facilities, without being judged by society.”
Kangemi Health Centre is not well equipped, has only three delivery beds
Barasa wants an adolescent-friendly booth with relatable services and staff who truly understand young people’s needs.
Barasa further noted that Kangemi Health Centre is not well equipped, as “Here we only have three delivery beds. Given the number of patients we serve, we are under-equipped. We have to refer other emergency cases if all of them are occupied at the same time.”

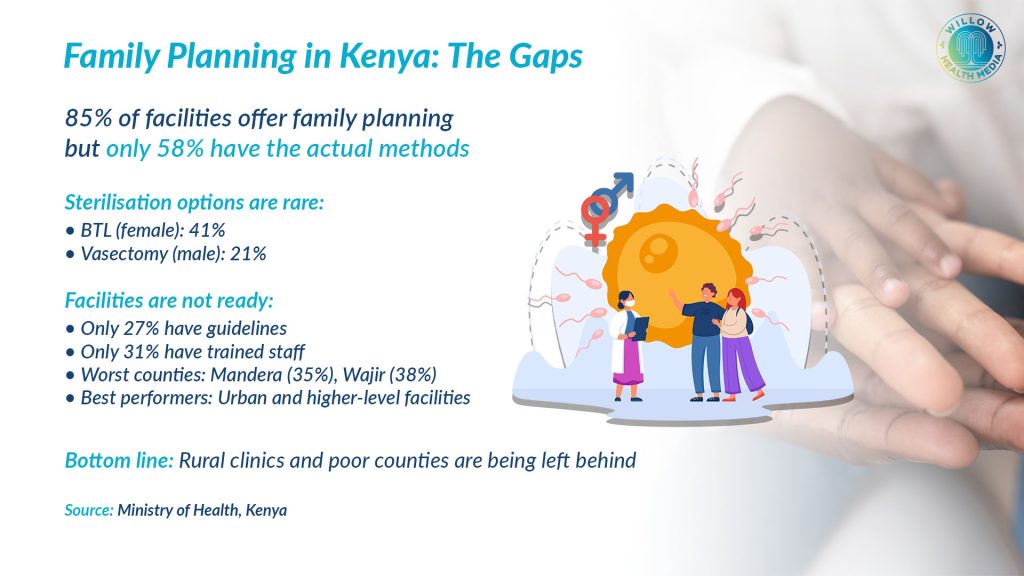
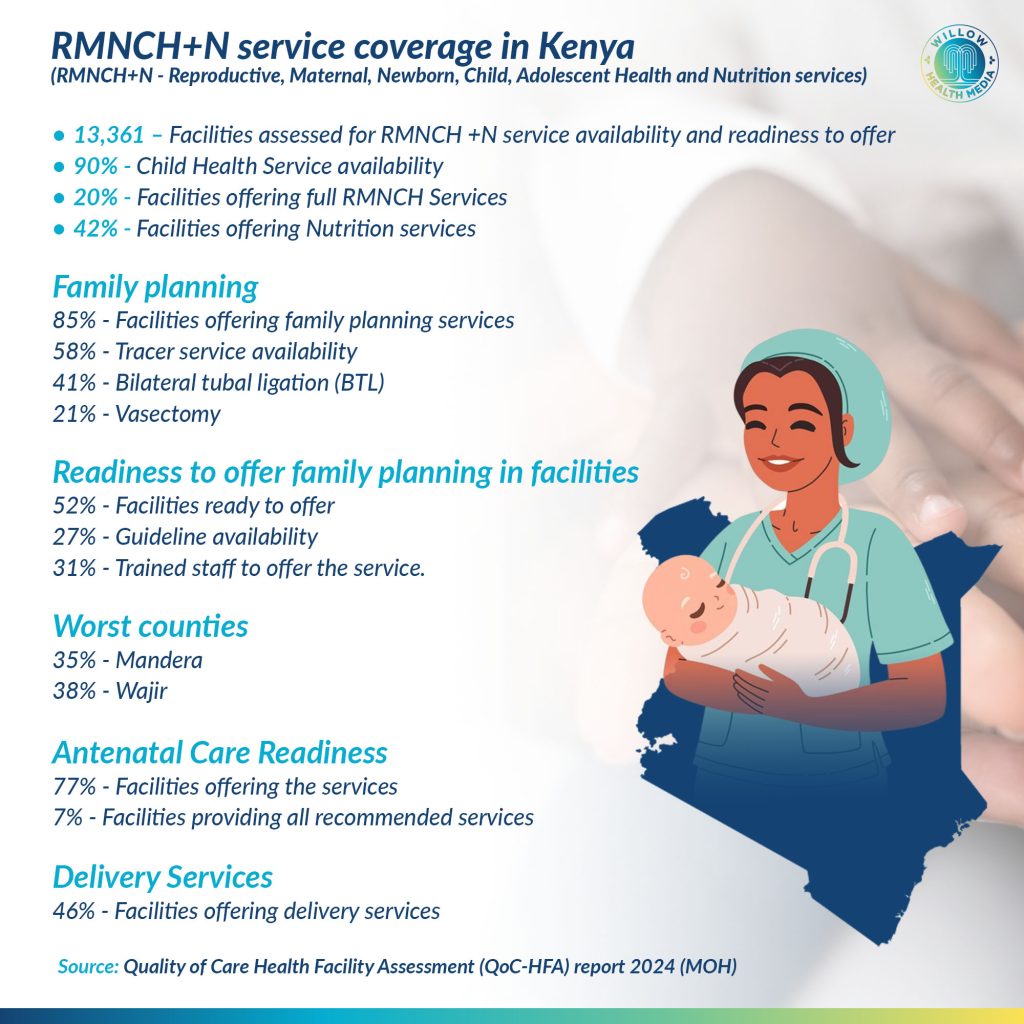
Her assertions reveal the dangers posed by gaps that were identified in the 2024 Quality of Care Health Facility Assessment (QoC-HFA) report. The Ministry of Health’s comprehensive survey confirmed critical gaps in reproductive, maternal, newborn, child, and adolescent health, and nutrition services (RMNCAH+N) across 13,361 facilities in all 47 counties.
The RMNCAH+N programme aims to eliminate preventable deaths while ensuring that women, children, and adolescents live healthy lives. Services begin from conception through pregnancy, childbirth, postpartum, infancy, and adolescence, covering preventive, curative, and rehabilitative interventions. However, despite this critical goal, the report notes that services are not adequately provided in most facilities as required.
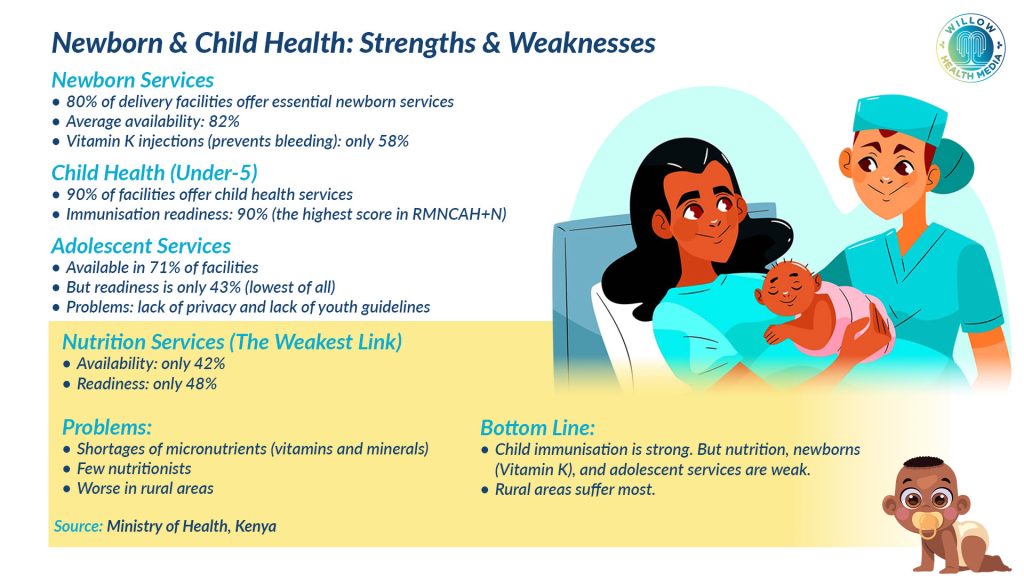
For example, while child health services lead in availability at 90 per cent, only 20 per cent of facilities offer the full RMNCAH package. Nutrition services lag at 42 per cent availability. These findings confirm persistent inequities, threatening Kenya’s Universal Health Coverage goals.
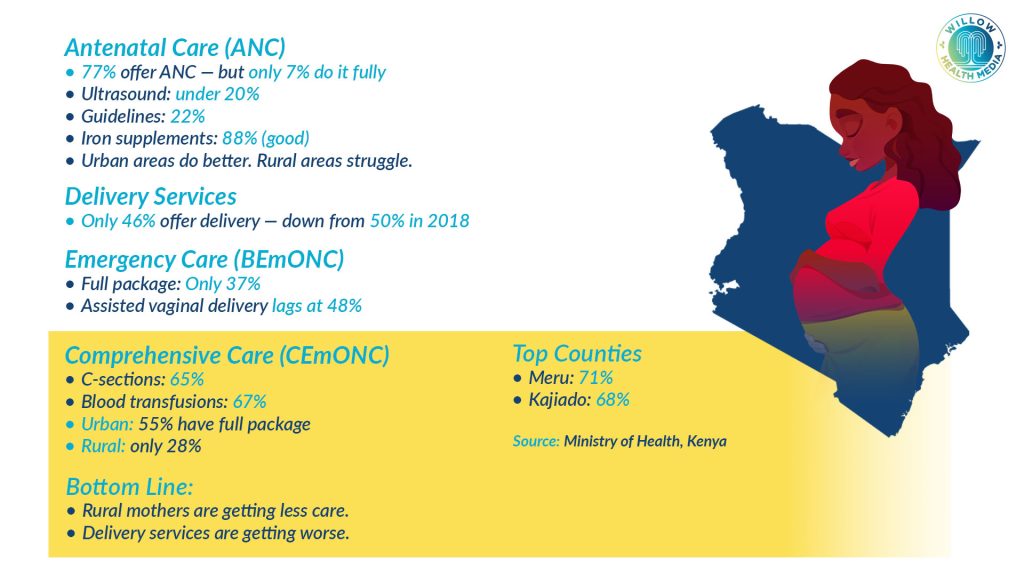
On antenatal care, more than half the facilities were found to offer the services, but a staggering seven per cent of the facilities were found to offer the full antenatal care services, highlighting rural and primary care deficits. Maternal Delivery Services were also found to be inadequate because more than half of the facilities were found not to offer delivery services.
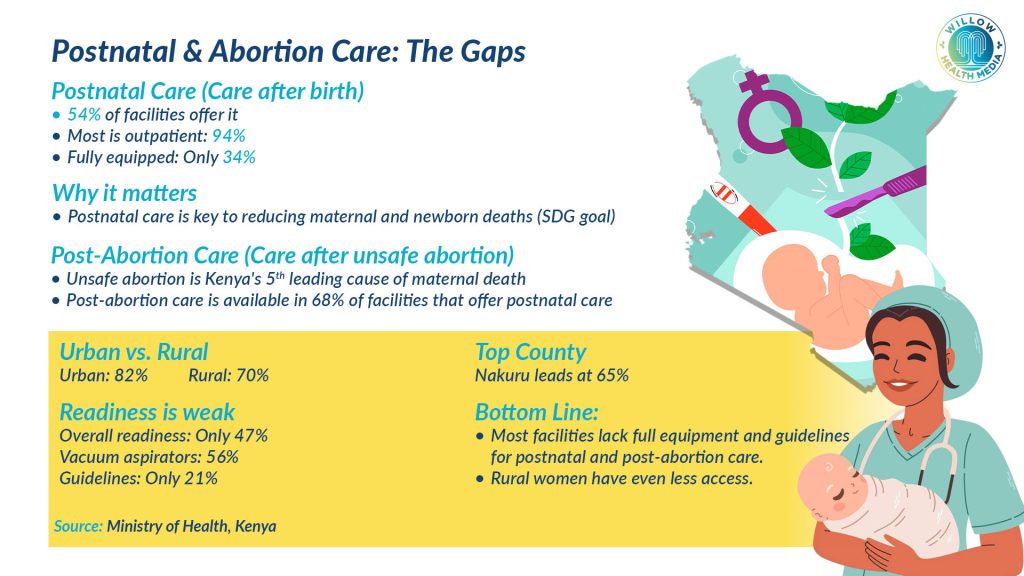
Postnatal care services are an important component of maternal and newborn health and also key to achieving the Sustainable Development Goals (SDGs) on the reduction of maternal mortality rates and end preventable deaths of newborns. However, postnatal care is provided in slightly over half of the facilities in the country.
Newborns require a wide range of medical and support measures to ensure their health and well-being, which include disease screening, vaccination, routine check-ups, and intensive care, among others. Despite being essential, newborn services are not available in all facilities, depriving newborns of the necessary nutrition services.
Uganda’s Emergency Obstetric and Newborn Care (EmONC) system faces severe challenges that continue to fuel preventable maternal and neonatal deaths, a senior government health official said at the International Maternal Newborn Health Conference 2026 in Nairobi.
Dr Ebong Chris, Senior Medical Officer at Uganda’s Ministry of Health, told delegates that the country’s struggles with Reproductive, Maternal, Newborn, Child, Adolescent Health and Nutrition (RMNCAH+N) are shared across the region, underscoring that the crisis is not unique to Kenya. He warned that human resource shortages, poor distribution of health workers, and institutional barriers continue to undermine service delivery, particularly in rural areas.
Uganda’s maternal mortality ratio (MMR) stands at 189 per 100,000 live births – above the Sustainable Development Goal targets -whilst the neonatal mortality rate (NMR) sits at 22 per 1,000 live births. Haemorrhage accounts for 42 per cent of maternal deaths, largely because many facilities lack critical EmONC functions such as blood transfusion and assisted delivery.
The country’s health system is tiered: Health Centre IIIs provide Basic EmONC (BEmONC) for catchment populations of around 20,000, whilst Health Centre IVs and district hospitals offer Comprehensive EmONC (CEmONC) – including surgical interventions – for larger populations. However, many facilities fall short of the required signal functions at both levels.
Investing in human resource via training, mentorship, recruitment, retention of midwives
Evidence cited by Dr Ebong illustrates what is achievable with improved services. The “CEmONC Availability Averts Deaths, Saving Mothers, Giving Life” initiative, commonly referred to as CAASML, reduced facility maternal deaths from obstetric haemorrhage by 42 per cent in Uganda through expanded services and increased access to caesarean sections. Alongside this, improved neonatal care cut neonatal mortality from 48 per cent to 21 per cent.

Dr Ebong cautioned that project-based funding, while helpful, should not be seen as a permanent fix. He urged sustained systems investment to protect mothers and newborns, arguing that lessons from funded programmes must be institutionalised rather than abandoned when external support ends.
To close the gaps, Dr Ebong proposed a multi-pronged approach: investing in human resource development through training, mentorship, recruitment and retention of midwives, anaesthesiologists and other essential personnel; phased annual upgrades of infrastructure and equipment; and stronger referral systems backed by improved ambulance services, transport networks, clear protocols and regional coordination centres. He also called for scaling up EmONC prioritisation nationwide to improve utilisation and access to life-saving care.
Graphics by Arthur Mbuguah.















