
One swab is all it takes. The test can protect you from cervical cancer for up to five years. It catches problems long before they become serious. The Social Health Authority (SHA) subsidises test for women aged 35 to 45.
Kenya is shifting from the Pap smear to HPV DNA testing, a more sensitive method that detects the virus behind most cervical cancers before abnormal cells even appear. This matters because cervical cancer kills about 3,600 Kenyan women a year, despite being largely preventable.
HPV DNA testing allows self-sampling and screening intervals of up to five years, though it costs three to four times more than a Pap smear and remains concentrated in private labs, mostly in Nairobi. Kenya’s Social Health Authority (SHA) now subsidises the test for women aged 35 to 45, and the country has built it into a new national elimination plan tied to global targets.
Why HPV DNA testing is different
For decades, screening has relied on the Pap smear, which involves collecting cervical cells and examining them under a microscope for abnormalities. According to Dr Jonathan Wawire, an anatomic gynaecologic pathologist at Aga Khan University Hospital, the Pap smear detects early cellular changes before they progress to cancer. “The Pap smear relies on collecting cells from the cervix, placing them on a slide, staining them, and examining them under a microscope,” he explains. “We look at the structure of the cells to identify any changes that may suggest progression toward malignancy.” This approach depends on visible changes, so early infections or risks may go undetected.

HPV DNA testing instead identifies the virus itself. “Over 90 per cent of cervical cancers are associated with high-risk HPV types,” Dr Wawire notes. “With HPV DNA testing, we are not waiting to see abnormal cells; we are directly looking for the presence of the virus itself.” The procedure is similar to a Pap smear: a swab sample is collected, but instead of being spread on a slide, it is placed in a preservative solution and sent for molecular analysis. The test detects DNA from high-risk HPV strains, particularly types 16, 18, and others linked to cancer.
A negative result means no high-risk HPV was found, so a woman can wait up to five years before the next screening. A positive result signals increased risk. “A positive HPV DNA test means the cells contain DNA from one of the high-risk HPV types,” Dr Wawire explains. “It does not mean the patient has cancer. It simply indicates a higher likelihood of developing it, which is why further evaluation is needed.” Follow-up may include a visual inspection of the cervix or a biopsy.
Ability to catch risk early
HPV DNA testing’s key strength is sensitivity, its ability to catch risk early. “HPV DNA testing will identify individuals who have the virus, even if there are no visible cell changes yet,” says Dr Wawire. The Pap smear, by contrast, is more specific.
“The Pap test can accurately identify those who likely have precancerous lesions,” he explains. “But it can also miss some cases. HPV testing, on the other hand, casts a wider net; it will catch more people at risk, including some who may not go on to develop disease.” That broader detection lets providers monitor and manage risk earlier.
Self-sampling expands access
A major advantage of HPV DNA testing is self-sampling. “With the Pap smear, it is difficult for a patient to collect a proper sample on their own because it requires reaching the cervix,” Dr Wawire explains. “But with HPV DNA testing, self-collection is possible using a swab.”

This could significantly expand screening coverage in underserved areas. The World Health Organisation supports self-sampling as a strategy to improve uptake, noting it increases convenience, cuts costs, and makes screening more accessible.
Samples are also stable once placed in preservative solution. “It doesn’t matter how long the sample takes to reach the lab,” Dr Wawire says. “The cells are well preserved, and the test can still be performed accurately.” Because HPV DNA testing needs specialised equipment and is often run in batches, results are not immediate. “In most cases, results are available within a week,” Dr Wawire notes.
Why age 30 is the starting point
WHO guidelines (2021) recommend starting HPV DNA screening at age 30. Dr Wawire explains: “Many people acquire HPV in their late teens or early twenties, but the immune system clears the infection in most cases.
If you test too early, you may find infections that would have resolved on their own, leading to unnecessary interventions.” By 30, persistent infections signal real risk. “For someone who still has high-risk HPV at that age, we begin to worry about persistence, which is associated with increased risk,” he adds.
Cost and access remain barriers
HPV DNA testing remains less accessible than the Pap smear across Kenya. Pap smears cost between Ksh1,000 and Ksh3,000, while HPV DNA testing costs three to four times more.

Yet Dr Wawire argues the long-term cost may be lower: “If you do a Pap smear every year, the cumulative cost over five years can exceed that of a single HPV DNA test, which only needs to be done once every five years if negative.” SHA now covers HPV screening for women aged 35 to 45 at a subsidised Ksh3,600 per test in eligible facilities.
Still, access is uneven. “Most of the facilities offering HPV DNA testing are private laboratories, many of them based in Nairobi,” Dr Wawire says. “For rural counties, access is still quite limited.” Uptake also depends on awareness, particularly around self-sampling. “It is a test that you may only need once every five years, which makes it quite acceptable to many patients,” he notes, though wider adoption will require more public education.
Kenya’s burden and policy response
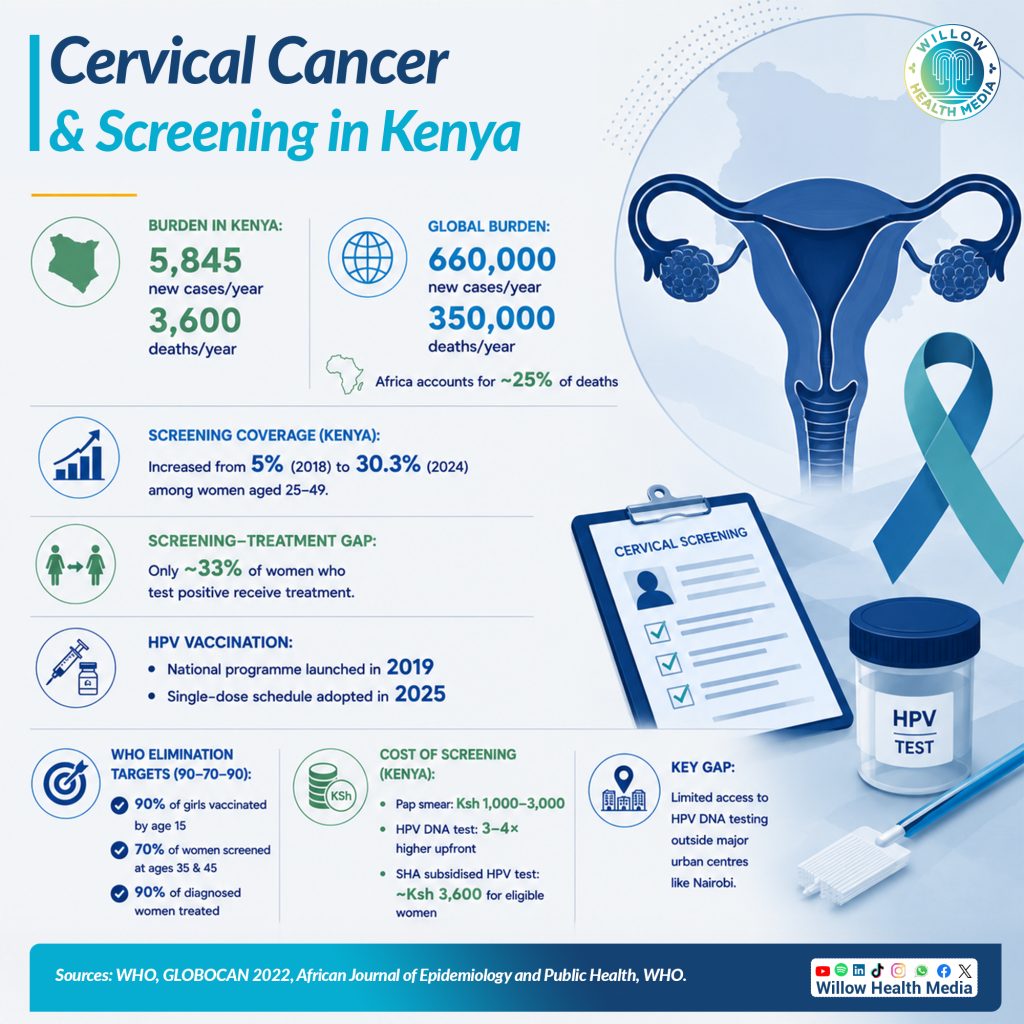
Cervical cancer remains one of Kenya’s leading causes of cancer death despite being largely preventable. GLOBOCAN 2022 data puts Kenya’s annual burden at about 5,845 new cases and 3,600 deaths. Globally, the disease causes around 660,000 new cases and 350,000 deaths a year, with Africa accounting for nearly a quarter of deaths. Experts say vaccination, screening, and treatment together can significantly cut this burden.

In 2026, Kenya launched the National Cervical Cancer Elimination Action Plan (2026-2030) with the WHO, aligned to global 90-70-90 targets: 90 per cent of girls vaccinated by age 15, 70 per cent of women screened at ages 35 and 45, and 90 per cent of diagnosed women treated. The national HPV vaccination programme began in 2019, moving to a single-dose schedule in 2025, and more than 11,000 health workers have been trained on vaccination and screening.
A 2026 study in the African Journal of Epidemiology and Public Health, on screening trends at Kiambu Level 5 Hospital, found cervical cancer screening coverage among women aged 25 to 49 rose from 5 per cent in 2018 to 30.3 per cent in 2024. Yet only about one in three women who test positive go on to receive treatment.
Looking ahead: Vaccination and timely treatment
HPV DNA testing is redefining cervical cancer screening through earlier detection and easier access via self-sampling. Combined with vaccination and timely treatment, it offers a real path to cutting cervical cancer deaths in Kenya.
But as Dr Wawire stresses, screening alone is not enough; identifying risk must be followed by diagnosis and treatment. With the right investment in infrastructure, awareness, and follow-up care, Kenya has the tools to make cervical cancer preventable and manageable. The challenge now is ensuring those tools reach every woman, wherever she lives.













