
Duale’s announcement comes just one day after a High Court in Nairobi temporarily blocked the Kenyan government from establishing a US-linked Ebola quarantine facility in the country.
The Government of Kenya has confirmed it is partnering with the United States government to establish a dedicated Ebola Virus Disease (EVD) isolation and treatment centre in Laikipia, a move officials say is aimed at strengthening surveillance, emergency response and treatment capacity amid the ongoing Ebola Virus Disease outbreak in Uganda and the Democratic Republic of Congo (DRC).
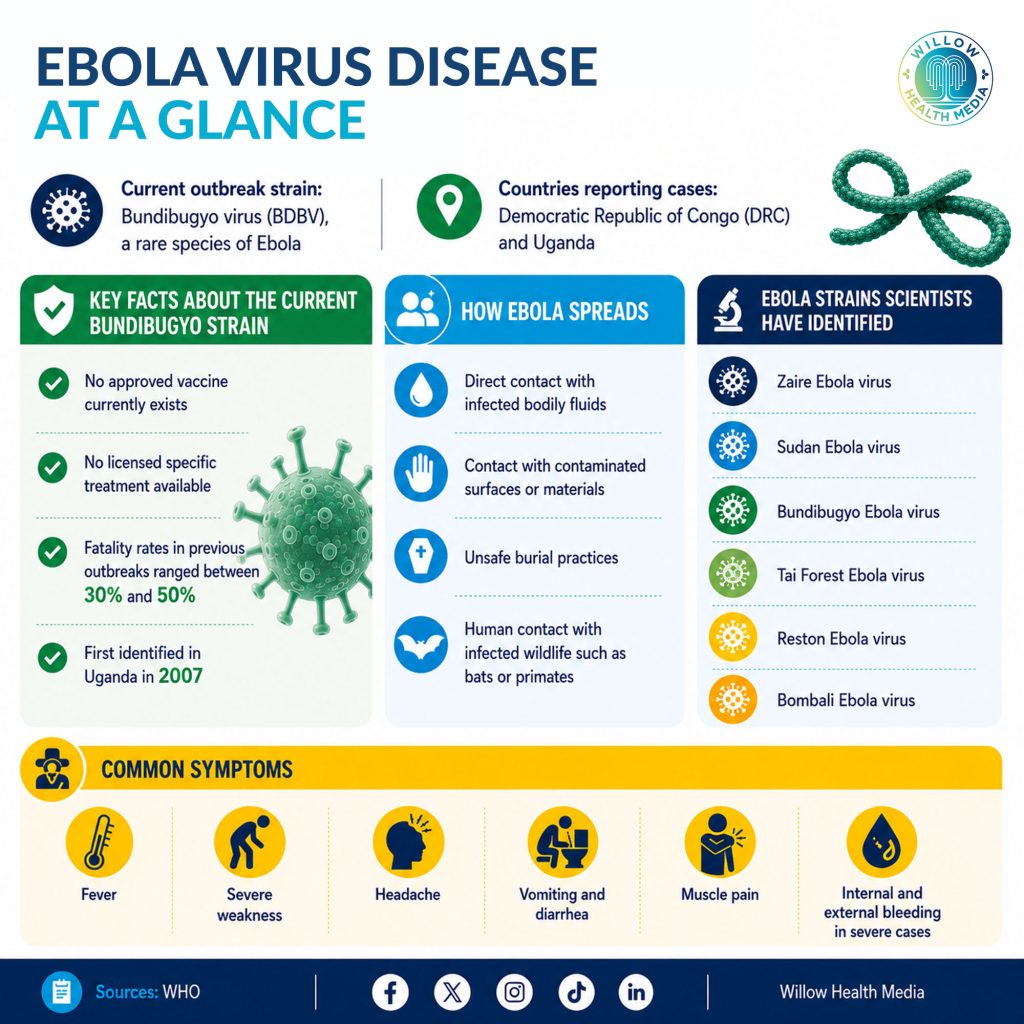
Health Cabinet Secretary Aden Duale yesterday said the partnership was catalysed by the spread of the Bundibugyo species of Ebola Virus in Uganda and the DRC, triggering a strain that currently has no approved vaccine or therapeutics.
“The partnership supports enhanced surveillance, diagnostic capacity, emergency preparedness exercises, critical medical supplies and rapid response capabilities,” Duale said in a statement issued on May 30.
He further stated that the treatment and isolation centre will be located within a military installation in Laikipia, while the Ministry of Health has also established additional Ebola isolation and treatment units at Kenyatta National Hospital, Moi Teaching and Referral Hospital in Eldoret, and the Kenya National Police Hospital.
Duale’s announcement comes just one day after a High Court in Nairobi temporarily blocked the Kenyan government from establishing a US-linked Ebola quarantine facility in the country, following a petition raising constitutional and public health concerns.
Justice Patricia Nyaundi on Friday, May 29, issued conservatory orders barring the government from establishing, operationalising, facilitating or approving any Ebola exposure, quarantine, isolation or treatment facility linked to the US or any foreign government, pending the hearing and determination of the case. The court also prohibited Kenya from admitting or facilitating the entry of persons exposed to or infected with Ebola under the disputed arrangement.
The orders were granted following a petition by Katiba Institute, which sued the Attorney General and the Ministry of Health, arguing that the alleged Kenya-US agreement was being pursued secretly and without constitutional safeguards, including public participation and parliamentary oversight. The case will be mentioned on June 2, 2026.
Kenya had tested 16 suspected Ebola samples, all of which returned negative
Duale’s announcement yesterday has triggered public anxiety, legal challenges and renewed scrutiny of Kenya’s fragile healthcare system, with critics questioning whether the country has sufficient resources, workforce capacity and infrastructure to safely manage an outbreak of such magnitude.
As of May 30, Kenya had tested 16 suspected Ebola samples, all of which returned negative.
“Please be advised that as of today, there are no confirmed cases of Ebola Virus Disease in the country,” Public Health Principal Secretary Mary Muthoni said after a situational assessment at Jomo Kenyatta International Airport (JKIA).
The reassurance, however, comes against the backdrop of a rapidly escalating regional outbreak that has placed East African health systems on high alert. The Ministry of Health has classified Busia, Bungoma, Trans Nzoia, West Pokot, Turkana, Migori and Homa Bay among the highest-risk counties due to their proximity to Uganda and regional movement patterns.
Other counties considered high-risk transit and commercial hubs include Nairobi, Mombasa, Kisumu, Uasin Gishu, Siaya, Kericho, Nakuru, Kiambu, Machakos, Makueni, Taita Taveta, Kilifi and Kwale.
According to outbreak data from the Institut National de Santé Publique (INSP), the outbreak in the DRC has recorded 1,031 confirmed and suspected cases and 240 confirmed and suspected deaths. Of these, 125 are confirmed cases while 906 remain suspected. The outbreak has also resulted in 17 confirmed deaths and 223 suspected deaths.
On May 17, the World Health Organisation (WHO) declared the outbreak a Public Health Emergency of International Concern (PHEIC), urging neighbouring countries to intensify surveillance, strengthen laboratory capacity and fast-track therapeutic approvals.
Unlike the Ebola-Zaire strain, which has approved vaccines developed by Russia’s Gamaleya Centre, the Bundibugyo strain currently lacks licensed vaccines or proven therapeutics, making containment heavily dependent on rapid detection, isolation and public health response systems.
For Kenya, the situation revives painful memories of Covid-19, when even relatively stronger health systems struggled under the weight of overwhelmed hospitals, oxygen shortages, workforce burnout and disrupted supply chains.
Kenya remains vulnerable to another large-scale outbreak, particularly one involving a highly fatal disease such as Ebola
The pandemic exposed longstanding structural weaknesses in Kenya’s healthcare system, including chronic underfunding, dependence on donor support, laboratory inequities between urban and rural counties, and insufficient emergency preparedness financing. It also demonstrated how quickly infectious diseases can destabilise economies, interrupt education, overwhelm hospitals and deepen social inequalities.
While Kenya ultimately avoided the worst Covid-19 mortality outcomes seen elsewhere, experts say the country remains vulnerable to another large-scale outbreak, particularly one involving a highly fatal disease such as Ebola.
Ebola outbreaks can carry fatality rates of up to 90 per cent depending on the strain and response speed, while healthcare workers remain among the most exposed populations during outbreaks.
That reality has fuelled public concern over Kenya’s decision to host an Ebola isolation and treatment centre linked to a US partnership, especially after reports emerged that the United States had tightened entry restrictions for travellers arriving from high-risk Ebola countries.
The US government has barred entry for visitors and citizens who have recently travelled to Ebola high-risk countries within the previous 21 days. Americans infected or suspected to have contracted Ebola are currently being treated in Germany and the Czech Republic rather than being repatriated to the US.
The development has intensified debate among Kenyan civil society organisations, some of which have already secured a temporary court injunction seeking to halt the plans. Critics argue that Kenya risks becoming a regional holding ground for infectious disease threats while still struggling with shortages of healthcare workers, medical supplies and financing for routine care.
But government officials insist the partnership is ultimately intended to strengthen Kenya’s own health security systems.
“Kenya must remain prepared to prevent, detect and respond to public health threats before they reach our communities,” Duale said. “Protecting Kenyans requires more than hoping diseases do not cross our borders or solely relying on screening at border points.”
The Health CS argued that investments linked to the partnership would leave behind long-term benefits for Kenya’s healthcare system, including improved laboratory infrastructure, stronger disease surveillance, emergency response systems, supply chains and workforce readiness.
Medical Services Principal Secretary Dr Ouma Oluga echoed the same position, saying Kenya had learned important lessons from Covid-19 and was now better positioned to respond to future pandemics. “Kenya prioritises the safety of its citizens, but we also cannot bypass opportunities to partner globally in ending outbreaks,” Oluga said earlier this week.
Kenya has further identified more than 10 border counties for additional preparedness measures
Kenya’s pandemic preparedness architecture has evolved significantly since Covid-19. The country has expanded genomic surveillance, strengthened airport screening systems, invested in rapid response teams and improved coordination between national and county governments during outbreaks.
The Ministry of Health says more than 100,000 Community Health Promoters (CHPs) now form part of the country’s frontline surveillance network, while digital disease monitoring systems have improved outbreak detection and reporting.
Kenya has further identified more than 10 border counties for additional preparedness measures as fears grow over cross-border transmission through trade routes, public transport corridors and informal movement along porous borders.
Yet major gaps remain. Kenya still relies heavily on donor-funded programs for disease surveillance, laboratory systems and emergency outbreak response. Counties continue to face persistent shortages of intensive care beds, isolation units, trained infectious disease specialists and personal protective equipment.
Public health financing also remains under strain amid broader economic pressures and rising healthcare demands. Even routine services such as maternal care, immunisation and chronic disease management continue to face interruptions during outbreaks, often disproportionately affecting poor and rural communities.
Health experts warn that fear and misinformation could also complicate Ebola preparedness efforts if public communication is not handled carefully. Muthoni urged health partners and media organisations to prioritise accurate public information and counter misinformation that could trigger panic or stigma. She said the Ministry of Health would convene additional stakeholder meetings to strengthen coordination and public awareness efforts.















