

The 2022 KDHS data shows three hard truths: rice farms may be harming pregnancies, urban women face higher miscarriage rates than rural women, and a border county’s high abortion rate reveals a broken reproductive health system.
Kirinyaga County has the worst pregnancy outcomes in Kenya, with a miscarriage rate nearly double the national average. The county sits on top of the Mwea Irrigation Scheme, the country’s largest rice farm, where unregulated pesticide use has left toxic residues in the soil and waterways. New data also reveals a striking and counterintuitive pattern: urban women in Kenya are losing more pregnancies than their rural counterparts, and educated women in wealthier counties are miscarrying at higher rates than women in some of the country’s most remote areas.

The miscarriage rate in Kirinyaga currently stands at 19.3 per cent, nearly double the national average of 9.8 per cent and the highest of any of Kenya’s 47 counties. Almost one in five recognised pregnancies in Kirinyaga end without a live baby. The county, located in the Central Kenya highlands, roughly 100 kilometres from Nairobi, has relatively high health facility coverage. It also hosts the Mwea Irrigation Scheme, 30,000 hectares of paddy fields that produce more than 80 per cent of Kenya’s domestic rice supply.
A 2024 study on Mwea’s soil, titled “Agricultural Pesticide Residue Levels in Soil from the Farms Along Thiba River Catchment Area, Mwea Irrigation Scheme, Kirinyaga County, Kenya”, detected significant residues of chlorpyrifos in the Thiba River catchment area. Chlorpyrifos is an organophosphate pesticide banned in several countries, and levels at some sites reached up to 213 micrograms per kilogram. Data from the 2022 Kenya Demographic and Health Survey (KDHS) shows a troubling pattern: the county with the country’s most intensive chemical farming also records the highest miscarriage rate in Kenya.
The risks are not confined to Kirinyaga. A 2022 report by Environmental Sciences Europe, titled “Women in Agriculture: Pathways of Pesticide Exposure, Potential Health Risks and Vulnerability in Sub-Saharan Africa“, found that in Kenya’s horticultural sector around Lake Naivasha, the burden of pesticide exposure falls disproportionately on women.

While 88.5 per cent of male workers were pesticide applicators, the majority of female workers, who were engaged in planting, weeding, harvesting and pruning, reported the highest rates of respiratory, skin, joint and nervous system symptoms. They were not spraying. They were simply working in fields where pesticides had already been applied, with little training and limited access to protective equipment.
Biology compounds the risk further. Women carry higher levels of adipose tissue on average and undergo hormonal changes during pregnancy, lactation and menopause that increase their capacity to absorb certain pesticides. Research cited in the review found that women exposed to pesticides experienced reproductive problems or birth defects in their children, and that spontaneous miscarriages and infant deaths have been recorded among female farmworkers exposed to chemicals, several of which fall under the World Health Organisation’s (WHO) most hazardous pesticide classifications.
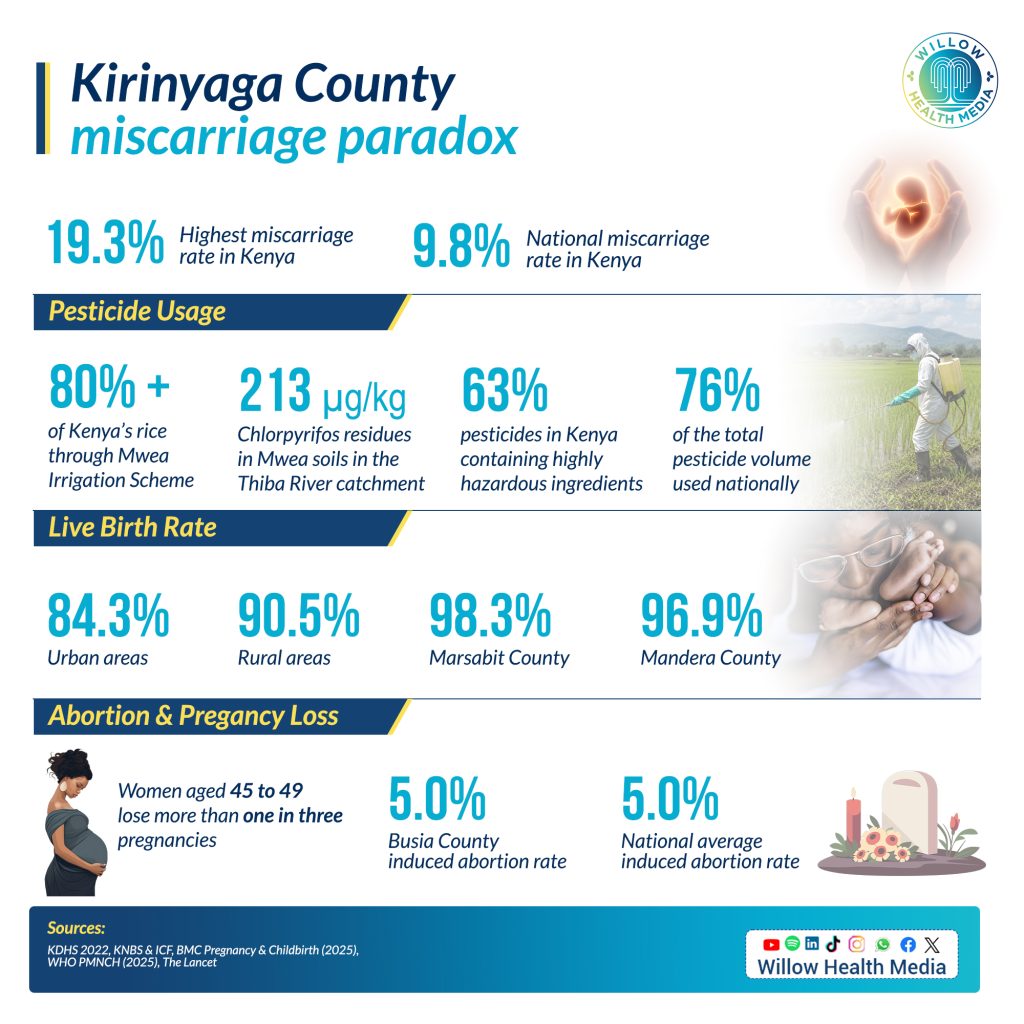
Kenya’s pesticide market has grown significantly, and the picture is alarming. A 2023 report titled “Toxic Business: Highly Hazardous Pesticides in Kenya”, published by the Route to Food Initiative and Heinrich Böll Foundation Kenya, found that of the 310 pesticide products in active use in 2020, 63 per cent contained active ingredients classified as Highly Hazardous Pesticides, accounting for 76 per cent of the total volume applied across the country.

Almost half of all pesticides used by volume are substances already banned in Europe due to unacceptable risks to human health and the environment. Among the most widely used are chlorpyrifos, mancozeb, paraquat and glyphosate, each carrying documented risks including reproductive toxicity, endocrine disruption and carcinogenicity.
What makes this particularly concerning for pregnant women and unborn children is the near-total absence of monitoring. A retrospective study at Kenyatta National Hospital (KNH) found that pesticide poisoning accounted for 43 per cent of all acute poisoning admissions, with organophosphates among the leading causes. Organophosphates are strongly associated with reproductive harm. Yet Kenya has no comprehensive network of poison control centres, the true number of acute poisonings each year goes unreported, and chronic health effects from long-term pesticide exposure, including those affecting reproduction, are not monitored at all.
Why city women are losing more pregnancies than rural ones
The 2022 KDHS data reveals a pattern that challenges assumptions about urban advantage in healthcare. Urban women have a live birth rate of 84.3 per cent, compared to 90.5 per cent for rural women, a gap of 6.2 percentage points. Urban women also miscarry at nearly double the rate of rural women. Nairobi records a live birth rate of just 84.5 per cent, while Kiambu records 81.3 per cent. Meanwhile, Marsabit, which is remote and pastoralist with limited hospital infrastructure, records the country’s highest live birth rate at 98.3 per cent, and Mandera posts 96.9 per cent.
The causes are multiple. Urban women tend to be older when they conceive, more likely to have delayed first pregnancies into their thirties, and more exposed to chronic stress, air pollution and sedentary lifestyles, all of which the Lancet’s miscarriage series identifies as independent risk factors. The survey also shows that the counties with the highest miscarriage rates are consistently the counties where women are most educated, most urban and most likely to have delayed first pregnancies: Nairobi, Kiambu, Kirinyaga and Nyeri. Kenya’s economic transformation is producing a generation of women entering their first pregnancy in their thirties.

Access to care is also fracturing along new lines. WHO’s Partnership for Maternal, Newborn and Child Health noted in 2025 that Kenya’s transition from the Linda Mama programme to the new Social Health Insurance Fund has disrupted maternity care access, with early signs of declining skilled birth attendance. That decline falls hardest on a middle tier of women who are neither wealthy enough for private care nor remote enough to have been consistently served by the old system. The 2022 DHS also shows that over one-third of Kenyan pregnant women still do not complete four antenatal visits, with only half of women with no education reaching this minimum compared to more than eight in ten with higher education.
Age is also a significant factor. The survey shows that women aged 45 to 49 lose more than a third of pregnancies to miscarriage. At under 20, the miscarriage rate is just 4 per cent, with a live birth rate of 93.3 per cent.
Busia’s abortion rate is eight times higher than Kenya’s national average
A separate pattern is emerging in Busia County, which records an induced abortion rate of 5.0 per cent against a national average of 0.6 per cent, eight times the national figure. Kenya’s constitution permits abortion only when a trained health professional deems it necessary for the life or health of the mother. In practice, the law is restrictive.
Busia, however, shares a busy border crossing with Uganda, where, while abortion law is similarly restrictive on paper, border-town pharmacies and informal providers operate with considerable practical latitude. Cross-border health-seeking is well documented across East Africa, particularly for reproductive and sexual health services that are stigmatised or legally risky at home.
Women with higher pregnancy orders face elevated risks of gestational diabetes, anaemia
The DHS data on pregnancy outcomes by birth order adds a further dimension. First pregnancies achieve a live birth rate of 92.2 per cent and a miscarriage rate of 5.5 per cent, the best outcomes of any group in the dataset. By the fifth or higher pregnancy, live births have fallen to 85.6 per cent, and miscarriage has climbed to 12 per cent.

Women with higher pregnancy orders face elevated risks of gestational diabetes, anaemia, uterine rupture and pregnancy loss globally and in Kenya specifically. Each subsequent pregnancy places greater physiological demand on a body that may also be ageing, nutritionally depleted or under-supported by the health system. Kenya’s family planning messaging has historically focused on reducing total fertility by encouraging smaller families through contraceptive use, but the data suggest the quality of care across all pregnancies deserves equal attention.
The evidence from Kirinyaga, from Kenya’s cities, and from the DHS as a whole points to a crisis in pregnancy outcomes that is poorly understood, inadequately monitored and urgently in need of a coordinated national response.













