
Kenya can no longer rely on yesterday’s strategies alone to fight today’s malaria threat, it must innovate, strategise, and prioritise.
For decades, we thought we knew the enemy in malaria prevention and control. We knew when it struck, where it hid, and who it targeted. But malaria is changing, and Kenya’s response must change with it. As we mark World Malaria Day under the theme, “Driven to End Malaria: Now We Can. Now We Must,” one thing is clear: Kenya can no longer rely on yesterday’s strategies alone to fight today’s malaria threat. It must innovate, strategise, and prioritise.

Approximately 579,000 malaria deaths occurred in the WHO African region in 2024, accounting for 95 per cent of malaria deaths globally. In places like Turkana County, families had lived with a sense of safety after years of declining case burden. The Kenya Malaria Strategic Plan 2019-2023 and the Kenya Malaria Indicator Survey 2020 classified Turkana as a seasonal semi-arid risk area with a prevalence of about one per cent. By 2015, there were no areas in Kenya where the parasite prevalence rate (PfPR2-10) exceeded 50 per cent, compared to 13.2 per cent of the population living in such areas in 2000, a remarkable sign of progress.
Today, the picture has changed dramatically. The Kenya Malaria Strategic Plan 2023-2027 now characterises Turkana as a high-burden endemic county with an adjusted incidence of 748 cases per 1,000 population. A new vector, Anopheles coluzzii, initially known to be restricted to West and Central Africa, has been detected at the Kakuma refugee camp in Turkana. Changes in vector behaviour, residual transmission, and shifts in species composition are driving a surge in severe and repeat malaria episodes. Recent analyses have shown these new vectors can increase malaria incidence by up to 50 per cent. Communities that once believed malaria was no longer a major threat are now facing new and growing risks, yet these vector behaviours remain insufficiently characterised for effective targeted interventions.
“Malaria is not only a rural problem. It is in our cities. It is in our deserts. It is on our doorsteps.”
One mosquito of growing concern is Anopheles stephensi, a malaria vector that thrives in urban environments. Unlike traditional malaria mosquitoes that breed in swamps and stagnant water, this species can breed in the shallow water found around homes, construction sites, water containers, and drainage systems in towns and cities. As urban areas in Kenya continue to grow, malaria could spread to places where people least expect it, including towns and cities not historically considered high-risk.
For years, Kenya’s malaria response was built on known mosquito species and established transmission patterns. Bed nets, indoor residual spraying, testing, and treatment remain essential tools that continue to save lives. But the emergence of new mosquito vectors and increasing resistance to commonly used antimalarials raises a critical question: are current interventions enough? They are necessary, but they are not sufficient on their own.
New tools for a new threat
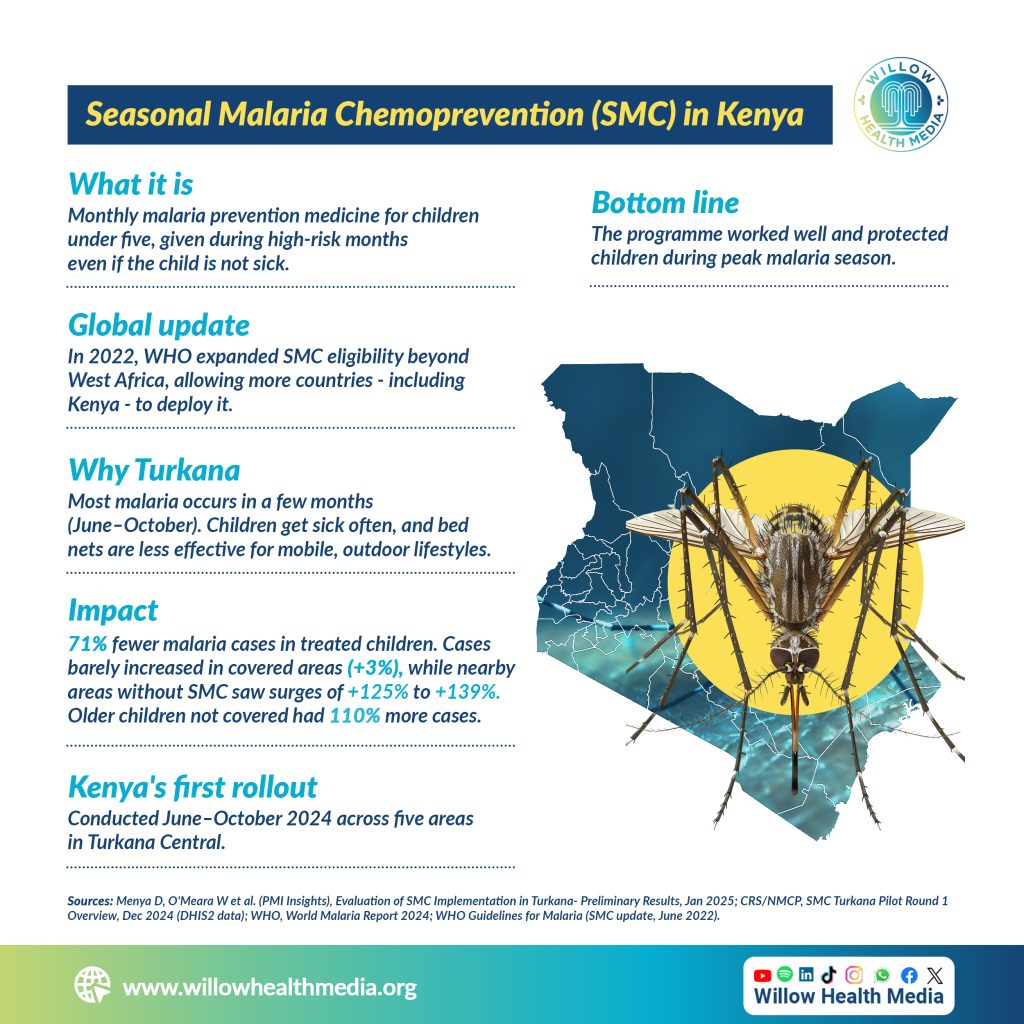
Kenya now has access to new tools that can help win the fight against malaria. One of the most promising is Seasonal Malaria Chemoprevention (SMC), in which children under five receive an antimalarial drug during peak transmission months to prevent infection before it happens. Kenya’s first SMC rollout in 2024, conducted from June to October across five areas in Turkana Central, yielded striking results: malaria cases among treated children fell by 71 per cent, with cases barely increasing in covered areas (+3 per cent), while nearby areas without SMC saw surges of 125 to 139 per cent.
Malaria vaccines are also offering new hope. The World Health Organisation has approved two vaccines, RTS,S and R21, marking an important breakthrough in the fight against malaria. The R21 vaccine is considerably more affordable: Gavi is purchasing R21 at US$2.99 per dose, compared to US$9.81 per dose for RTS,S. R21 has shown strong efficacy, reducing clinical malaria by 75 per cent in highly seasonal transmission settings and 68 per cent in areas with perennial transmission in clinical trials among African children.
Its greatest promise lies in combining it with SMC. Trials in Burkina Faso and Mali pairing seasonal vaccination with SMC demonstrated a reduction in clinical malaria by 63 per cent, severe malaria hospitalisations by 71 per cent, and malaria deaths by 73 per cent compared with SMC alone. Mathematical modelling confirms that pairing a pre-erythrocytic vaccine with SMC consistently outperforms either intervention deployed alone throughout childhood, with the largest gains in settings where SMC coverage is incomplete, precisely the situation in highly seasonal transmission areas such as Turkana.
What must be done
People are still dying of malaria in the 21st century, a disease we have all the tools to control and eliminate. Having the right tools is only half the battle. The other half is political will and investment to scale them up. The government must scale up interventions such as SMC and vaccines in all eligible counties and sub-counties where they will save the most lives, prioritised by data and sub-national targeting.

It must build domestic financing and reduce dependence on donor funding to create sustainable health systems capable of withstanding the kind of aid withdrawals recently witnessed across the globe. It must invest in robust entomological and public health surveillance systems, ones responsive enough to detect new vectors early, understand how malaria dynamics are shifting, and mount an effective response before outbreaks spiral out of control.
We owe this to every mother who has stayed awake through the night beside a sick child. To every family that has buried someone they did not have to lose. To every child who deserves to grow up without malaria as a fact of life. We have the solutions. We have the data. We have the science. What we need now is the urgency to fund it, scale it, and refuse to accept that any Kenyan child should die from a disease we know how to prevent.
The time to end malaria is not someday. It is now.
Now We Can. Now We Must.
Dr Geoffrey Githinji is a Research Fellow for Malaria Interventions Modelling at the Centre for Epidemiological Modelling and Analysis (CEMA), University of Nairobi. geoffrey.githinji@cema.africa















