


A University of Nairobi professor asked why so many women still died from something medicine already knew how to prevent. The answer changed maternity care across four countries.
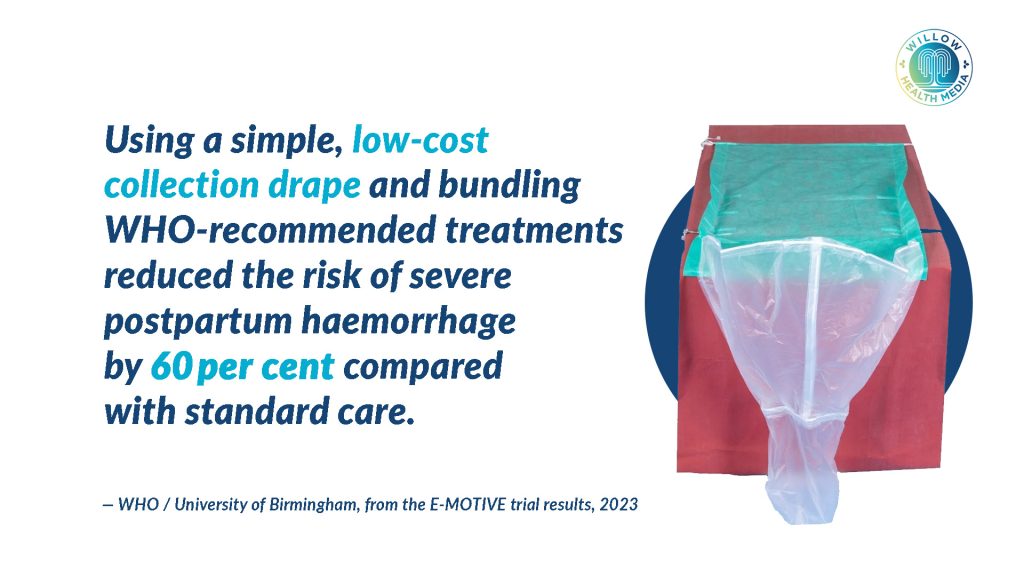
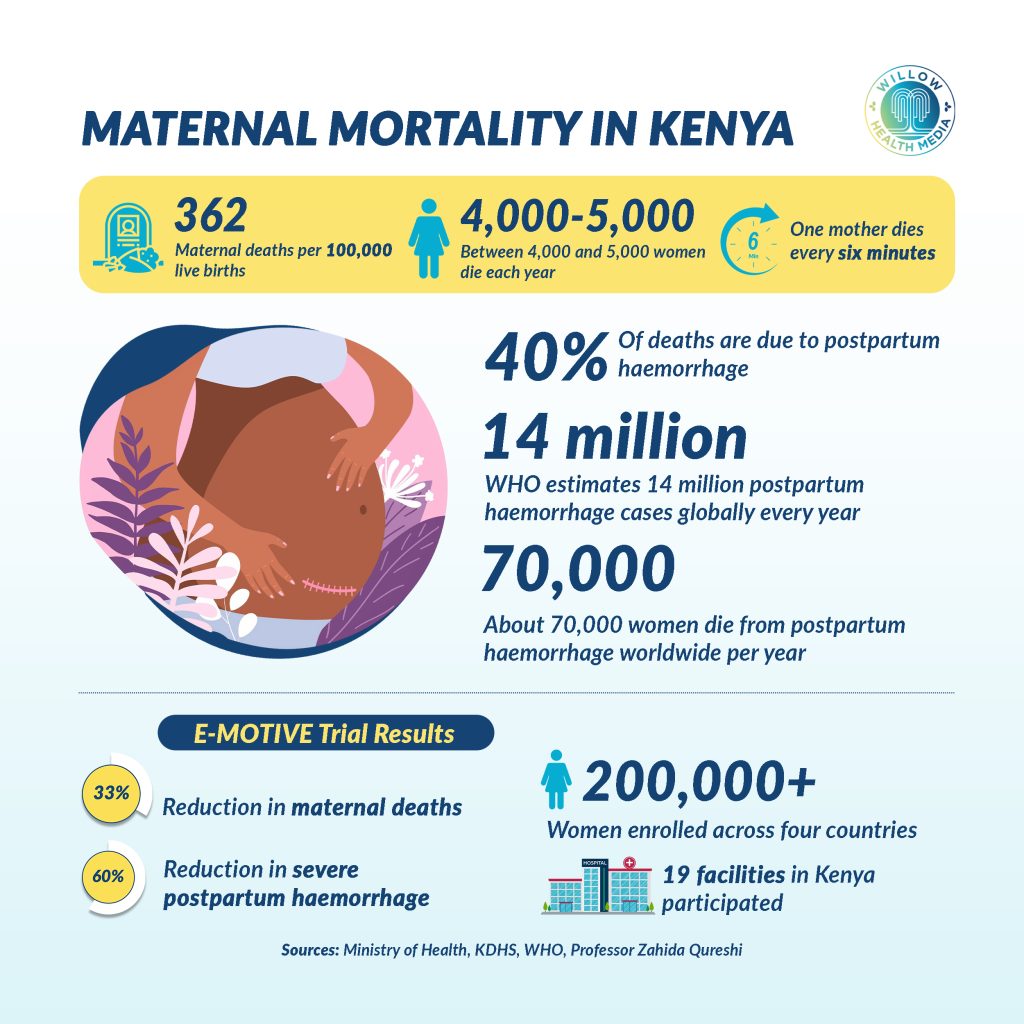
Every six minutes, somewhere in the world, a mother dies from postpartum haemorrhage. In Kenya, this preventable tragedy claims roughly 6,000 women every year, or about 16 mothers daily, women who never return home from the delivery room, leaving behind grieving families and motherless children. But across maternity wards in Kenya, a quiet revolution is unfolding, driven by a low-cost plastic drape with measurement markings that has reduced severe bleeding by 60 per cent and cut maternal deaths dramatically in facilities where it has been adopted.
Asnart Ouko, 28, knew her second pregnancy carried risks. Throughout it, even the slightest strain made her bleed. “If I worked a little or strained, I would bleed,” she recalls. Doctors warned her to slow down and attend clinic regularly for monitoring.
When she went into labour at Malindi Sub-County Hospital in 2024, her baby arrived within two hours. The speed of the delivery, a doctor later explained, was why her bleeding would not stop. When she started haemorrhaging, nurses quickly placed the PPH drape beneath her.

The drape showed she had lost over 500ml of blood, immediately confirming a dangerous postpartum haemorrhage. “If they hadn’t used that drape, they wouldn’t have known how much blood I lost,” she says. “It helped save my life.” After several hours of medication and careful monitoring, the bleeding slowed and she stabilised. She is now recovering, holding her newborn baby.
The calibrated PPH drape is a plastic sheet placed under the woman’s lower back during delivery, with a V-shaped pouch that collects and measures blood loss. It was created by Prof Zahida Qureshi, Head of the Department of Obstetrics and Gynaecology at the University of Nairobi, who spent years trying to answer one haunting question: why do so many mothers still die from something we know how to prevent?
The answer, she discovered, lay in something deceptively simple: estimation. In busy maternity units, healthcare providers would glance at the blood around the delivery area and make a quick visual judgement.
“One midwife might guess 200 millilitres. Another might guess 400. In reality, it could be 700 or more,” Prof Qureshi explains. “We were always underestimating. Once you give a number below 500, it means nothing is wrong. Intervention is delayed.”
By the time severe bleeding was recognised, women had often lost far more blood than anyone realised
There was another factor at play. “Healthcare providers don’t want to say they have a patient that has had postpartum haemorrhage because it’s like, ‘Oh, you didn’t manage her properly,'” Prof Qureshi notes. “So, you would always give a figure that is less than 500.” By the time severe bleeding was recognised, women had often lost far more blood than anyone realised.

Kenya’s maternal mortality ratio currently stands at 355 deaths per 100,000 live births. According to the Ministry of Health, PPH accounts for 25 to 45 per cent of maternal deaths nationally and is the leading cause of maternal mortality in the country. Globally, the World Health Organization (WHO) reports that 14 million women experience postpartum haemorrhage every year, and about 70,000 die, mostly in low and middle-income countries.
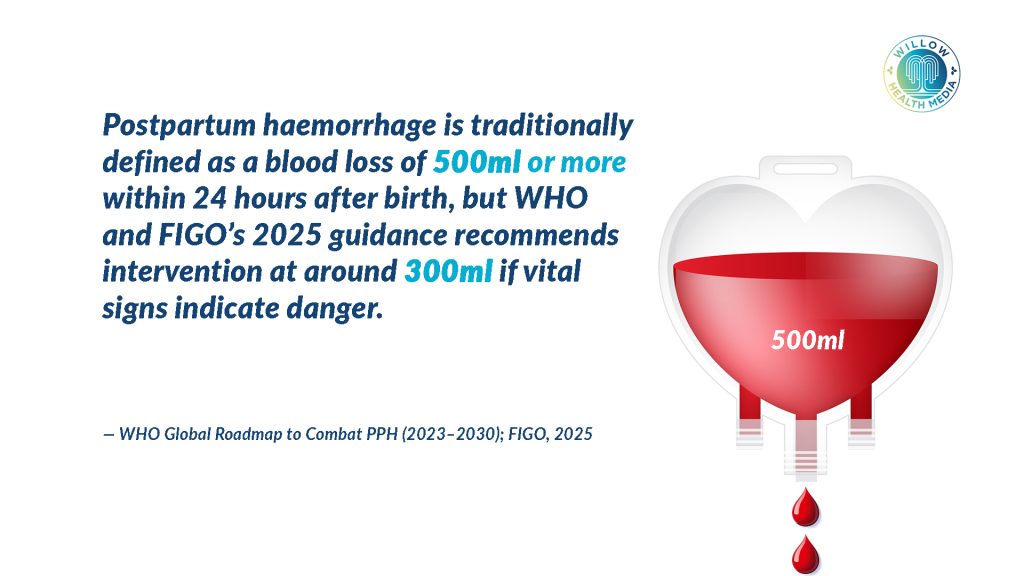
During delivery, blood funnels into the drape’s V-shaped pouch, which carries clear measurement markings at 300ml and 500ml. “When blood reaches 300 millilitres, it triggers an alert,” Prof Qureshi explains. “At 500 millilitres, treatment is mandatory.” Global health experts have since lowered the threshold to 300 millilitres following new guidance from the WHO, the International Federation of Gynaecology and Obstetrics, and the International Confederation of Midwives.

The drape works alongside the E-MOTIVE protocol, which stands for Early detection, Massage, Oxytocic drugs, Tranexamic acid, Intravenous fluids and Examination. Rather than trying one intervention at a time and waiting to see whether it worked, the protocol requires healthcare teams to perform all critical actions within 15 minutes. “Previously, we would try one thing then wait five to ten minutes,” Prof Qureshi says. “In this bundled approach, you do everything within 15 minutes.”
The urgency becomes clear when you understand what Prof Qureshi calls the golden hour. If postpartum haemorrhage is recognised and treatment begins within the first hour, survival is near 100 per cent. If recognition takes almost 60 minutes and treatment begins only after that, survival drops to between 10 and 20 per cent.
Researchers hoped to achieve 25 per cent reduction in postpartum haemorrhage, but achieved 60 per cent
The E-MOTIVE trial was conducted across 19 facilities in Kenya, Nigeria, Tanzania and South Africa. The researchers had hoped to achieve a 25 per cent reduction in severe postpartum haemorrhage. Instead, they achieved 60 per cent. “We all jumped up and down because we didn’t think it would be such a high figure,” Prof Qureshi recalls.

The impact at the facility level has been equally striking. At Malindi Sub-County Hospital, one of Kilifi County’s busiest maternity units, managing between 400 and 450 deliveries monthly, the numbers tell a clear story.
Mary Kariuki, Head of the Maternity Unit, said PPH used to be inconsistently managed. “Before the introduction of the drape, the PPH rate was about 5.3 per cent of the deliveries we used to conduct, and the death rate was about 1.8 per cent,” she said.
“But now after the drape was introduced, we were able to reduce it to about 3.4 per cent and the death rate to 0.02 per cent.” She added, “It has built our confidence. We realised mothers do not have to die from PPH when we can prevent it.”
In Kilifi County, where PPH accounted for 36 per cent of maternal deaths according to the 2024/2025 Maternal and Perinatal Death Surveillance and Response report, the county has introduced additional interventions, including 140 anti-shock garments, heat-stable carbetocin, uterine balloon tamponades and additional contractual maternity staff. Kilifi has since improved its ranking from 7th to 13th among counties with the highest maternal mortality.
When the drape was first introduced, some midwives resisted, fearing it would slow them down in already busy wards. Prof Qureshi and her team persisted, training staff and working alongside hospital teams. Once staff began using it, attitudes shifted quickly. “All the blood actually comes into the drape, and at the end of that one hour, you just pick it, and the whole place is just clean,” Prof Qureshi says. By the time the trial was ending, facilities were asking where they could order more. “They didn’t want to part with it,” she recalls.
Makueni County now reports zero preventable postpartum haemorrhage deaths
An unexpected breakthrough came when a Kenyan entrepreneur, having heard a woman describe her experience with the drape, set up a local factory to manufacture them. This solved a critical supply problem since drapes had previously been imported from India at high cost.

Kenyan hospitals can now order them at a reasonable cost through the Kenya Medical Supplies Authority. The manufacturer has developed three versions: a standard single-use drape, a biodegradable option, and a hybrid model where the top portion is reusable up to 100 times while only the collection pouch is discarded.
Nigeria has followed Kenya with local manufacturing. Ethiopia has sent observation teams. Tanzania and South Africa are developing their own scale-up plans.
WHO and the Gates Foundation have created a training package based largely on the E-MOTIVE model that any country can adapt and roll out. Kenya’s national guidelines have been updated, and the calibrated drape has been integrated into all emergency obstetric care training.
For Prof Qureshi, real impact comes when research becomes routine practice. For Asnart Ouko, the calibrated PPH drape was not just a medical tool. It was the reason she survived to be a mother to yet another child.
Graphics by Brian Wekesa.















Invention of drapes really saves lives because it helps in early identification of PPH which leds to early interventions.
Kongole kwa Professor Zahida for this good intervention 🥂. But the question is…. do we have enough drapes in our health care facilities for our mothers..?
Kuna hizi dispensaries which also conducts deliveries do they have drapes … ama drapes are only available for level 4 and 5 facilities pekee..?