
Previous annual cover for Sickle Cell was Ksh8,000 and ran out in two to three months, but now patients get Ksh20,000 for platelet treatment and Ksh70,000 for red cell exchange, each up to three times per year.
For years, sickle cell disease in Kenya has carried the double burden of pain and poverty, trapping families in endless cycles of blood transfusions, emergency admissions and impossible medical bills.
But now the revised Social Health Authority (SHA) package has expanded coverage for specialised sickle cell treatment, thus offering many families financial relief after Health Cabinet Secretary Aden Duale announced new covers for apheresis platelets at Ksh20,000 and red cell exchange at Ksh70,000, each available up to three times within a policy period.

The changes were gazetted on May 8, 2026, and replaced the previous annual allocation of just Ksh8,000, an amount families say lasted no more than two to three months before the cover ran out.
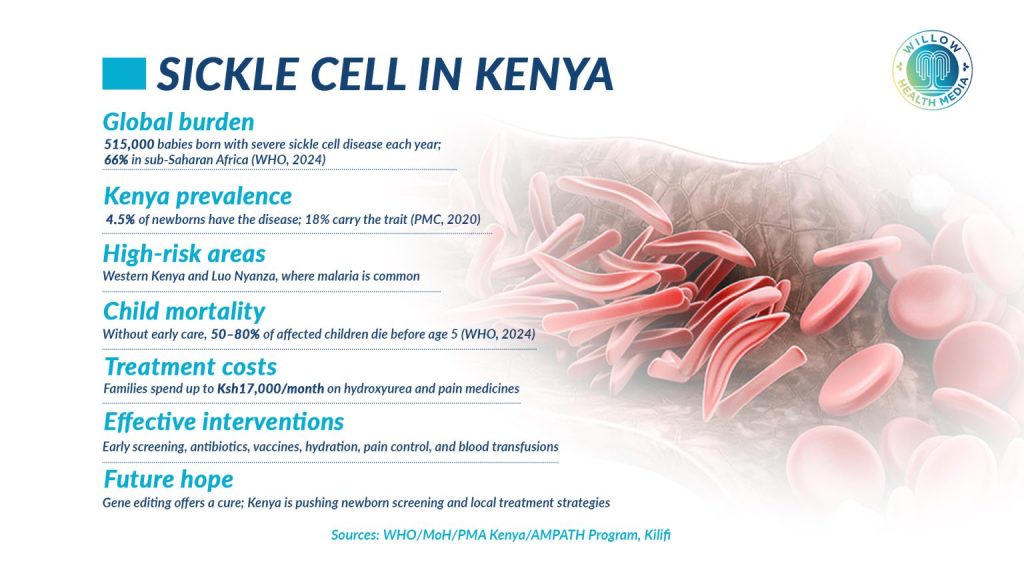
The disease remains heavily concentrated in Western, Nyanza and coastal Kenya, affecting at least 17 counties. The Ministry of Health (MoH) estimates that at least 14,000 children are born with sickle cell disease in Kenya annually. Across Sub-Saharan Africa, between 50 and 90 per cent of affected children die before their fifth birthday due to delayed diagnosis and limited access to treatment.
For families managing the disease daily, those numbers are not statistics. They are lived realities.
For families with more than one child living with sickle cell, the burden can be crushing
Mothers count tablet after tablet. Fathers wait outside hospital pharmacies late into the night, counting crumpled coins. A single Hydroxyurea tablet, one of the key medicines used to prevent severe complications, costs about Ksh70 in Kenya. Taken three times daily, it alone costs more than Ksh6,000 per month for one patient. Paludrin, another essential drug, adds roughly Ksh1,000 monthly. That is before factoring in transport costs, blood transfusions, emergency admissions and repeated hospital visits. For families with more than one child living with the disease, the burden can be crushing.

Caroline Mabunde, director of Don Amolo Memorial Kids Ark (DAMKA), an organisation supporting children living with sickle cell disease in Western Kenya, says the new package is welcome, but more is still needed.
“This is a big step in the right direction,” she says. “We will keep pushing for more comprehensive support because initially, the government had allocated a paltry Ksh8,000 annually under SHA for sickle cell treatment. That amount could only help for about two or three months before the cover was depleted.”
She adds that many patients still struggle to access Hydroxyurea and Paludrin despite their importance. Both drugs are critical in preventing severe complications and recurrent crises, yet they remain out of reach for many families managing costs on their own.
For scientists and clinicians, the revised package signals something larger than expanded financing. Phionah Obanda, a genomic scientist and member of the Sickle Cell Federation of Kenya, says the reforms mark a turning point in how the country treats the disease.
Sickle cell patients frequently face severe anaemia, stroke, organ damage and recurrent crises
“This revision is a significant breakthrough for sickle cell care in Kenya because it moves treatment closer to what patients actually need clinically, not just what is cheapest administratively,” she says.

Obanda explains that sickle cell disease is not a simple condition. Patients frequently face life-threatening complications, including severe anaemia, stroke, organ damage and recurrent crises, many of which require advanced procedures that were previously too expensive for most families.
“Red cell exchange can be lifesaving, especially for children and young adults facing acute chest syndrome or stroke complications,” she says. “Allowing access up to three times within a policy period could substantially reduce preventable deaths, long hospital stays and long-term disability.”
Yet even as families welcome the reforms, healthcare experts warn that money alone will not fix the deeper problems surrounding sickle cell treatment in Kenya. The country’s public health infrastructure, particularly in rural and county-level facilities, remains ill-equipped to deliver the very procedures the new package now funds.
Dr Roselyne Abwalaba, a lecturer in paediatric nursing and child health at Masinde Muliro University of Science and Technology (MMUST) and co-investigator in a sickle cell screening programme in Kakamega County, puts it plainly.
Without diagnostics, transfusion safety and specialist care, patients in rural Kenya may still struggle to benefit
“The next challenge is ensuring county referral hospitals have the infrastructure, trained personnel, blood supply systems and functional apheresis machines needed to deliver these services equitably,” she says. “Without investment in diagnostics, transfusion safety and specialist care, many patients in rural Kenya may still struggle to benefit from these reforms despite the expanded package.”
Apheresis machines, which are required to carry out the red cell exchange procedure now covered under SHA, are specialised and expensive. Many county hospitals do not have them. Without them, the new benefit remains, for many patients, a promise on paper.

That gap between policy and practice is already pushing new efforts on the ground. In Kakamega County, a two-year initiative called “Saving Newborn Lives Through Sickle Cell Disease Newborn Screening” is working to catch the disease at birth, before complications have a chance to take hold.
Early diagnosis leads to early care, and early care saves lives
The programme, a collaboration between DAMKA, MMUST and the Kakamega County Government, aims to screen 30,600 newborns across 21 hospitals using the HemoTypeSC point-of-care test, which produces results in about 10 minutes.
Children identified with possible sickle cell disease will receive free confirmatory testing and be enrolled into long-term care. Families will also receive free genetic counselling.
Dr Beatrice Mukabana, the project’s principal investigator, says the stakes could not be higher. “Sadly, between 50 and 90 per cent of these children die before reaching their fifth birthday, largely because of late diagnosis and delayed initiation of care. Through early screening, we are able to detect the condition at birth, begin care immediately and significantly reduce complications and deaths.”
Livingstone Imbayi, the Kakamega County Executive Committee Member for Health, says the message is straightforward. “Early diagnosis leads to early care, and early care saves lives.”
Graphics by Brian Wekesa.















