
What happens when patients arrive early, but hospitals aren’t ready, the insurance fails, and the machines are silent? Kenya’s cancer crisis has an answer.
Kenya’s fight against cancer is being seriously undermined by late diagnosis, dysfunctional payment systems, cultural barriers and fragmented efforts – even as insurance coverage improves and more patients seek treatment. These findings emerged at a World Cancer Day seminar hosted by the Kenya Society of Haematology and Oncology (KESHO) in February 2026.
The most alarming finding is how long Kenyans wait for a cancer diagnosis. Dr Ouma Oluga, Principal Secretary for Medical Services, cited the 2025 quality of care report, which found that most cancer patients took five months before receiving an accurate cancer diagnosis. For context, the National Health Service (NHS) in the United Kingdom requires that patients either receive a diagnosis or have cancer ruled out within 28 days, under its Fast Diagnostic Standard introduced in 2023.

Critically, Dr Oluga challenged the common assumption that Kenyans present to hospitals too late. “Patients visit hospitals early, but the facilities they visit have low cancer suspicion rates and lack proper testing equipment. Patients don’t trust them either. They get a diagnosis after interactions with many facilities,” he said. Each additional visit delays diagnosis further and drains patients financially. “Cancer can make you poor or make you die. Most patients get a diagnosis when they have depleted their covers. It is a bad experience with bad outcomes for our patients,” Dr Oluga warned.
To address the equipment gap, the government has launched the National Equipment Service Programme and purchased 84 mammograms for six public cancer centres and other hospitals nationally to accelerate breast cancer detection.
On the financing side, Kenya’s Social Health Authority (SHA) has expanded cancer coverage significantly compared to its predecessor, the National Health Insurance Fund (NHIF). Dr Diana Marion, SHA Director of Provider and Beneficiary Management, outlined the current structure: cancer is covered across three tiers – primary healthcare (PHC), the Social Health Insurance Fund (SHIF), and the Emergency, Chronic and Critical Illness Fund (ECCIF).
Under SHIF’s enhanced oncology cover, chemotherapy is covered at Ksh5,500 per session
Under PHC, which is fully government-funded, patients can access diagnostic tests and some surgical procedures. Under SHIF’s enhanced oncology cover, chemotherapy is covered at Ksh5,500 per session and radiotherapy at Ksh3,600 per session. The overall coverage limit was raised from Ksh150,000 to Ksh400,000, with ECCIF contributing an additional Ksh400,000, bringing the total to Ksh800,000. Cervical cancer treatment through brachytherapy is covered at Ksh40,000 for two sessions, and stereotactic body radiation at Ksh70,000. ICU care under ECCIF is covered at Ksh28,000 for up to 21 days.
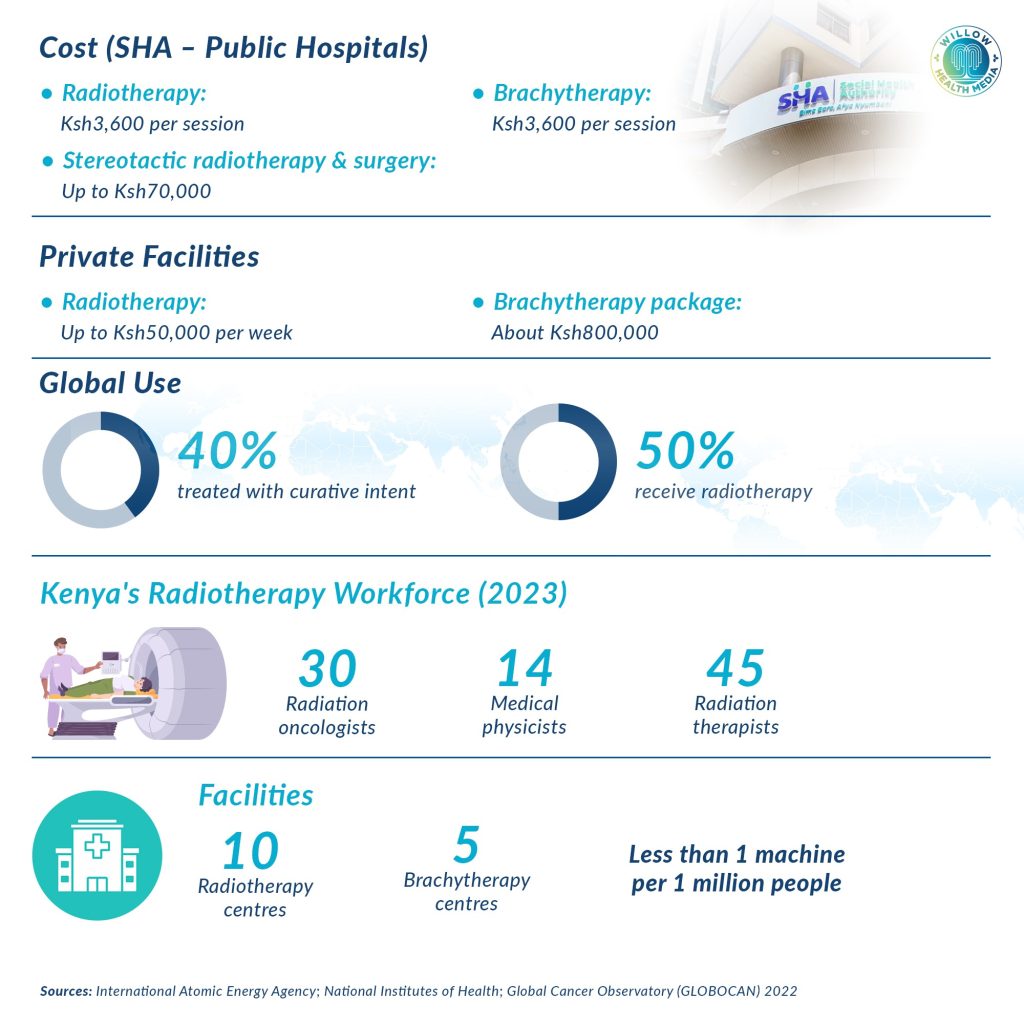
The impact has been measurable. “From October 1, 2024, we have paid cancer treatment claims of Ksh7.5 billion for 43,561 patients in over 140 registered facilities,” Marion said. At Nairobi Hospital, Dr Gladwell Kiarie from KESHO reported that the number of patients receiving radiotherapy rose from 30 per day under private insurance and out-of-pocket payments to over 70 per day since SHA introduced its package.
A notable milestone is the co-financing agreement between SHA and Roche, the global biotechnology company, which has subsidised Herceptin – a vital breast cancer drug administered in 16 cycles – from Ksh350,000 to Ksh33,000. In May 2025, the Ministry of Health announced that the broader partnership with Roche would lower breast cancer treatment from Ksh120,000 to Ksh40,000 per session, with no co-payment required from patients.
Despite these gains, serious cracks remain. Prisca Githuka, chairlady of the Cancer Survivors Association of Kenya and a breast cancer survivor, welcomed the improved cover but was direct about its shortcomings. “SHA should, however, be comprehensive and uninterrupted. Most patients are dropping out of treatment because they are turned away by facilities that haven’t been reimbursed by SHA. Public facilities, unable to operate, are referring patients to private facilities, which are expensive and stress patients further,” she said.
Githuka also pointed to a fundamental infrastructure problem: “The hospitals should also be equipped to better diagnose and treat patients. It’s a reverse of gains for one to have an oncology cover only to get to the Kenyatta National Hospital and find the radiotherapy machine isn’t working.”
Pending government bills cripple basic functions, including blood transfusions at major cancer centres
The financial strain on public facilities compounds the problem. Seme MP Dr James Nyikal, who chairs the National Assembly’s Health Committee, said pending government bills regularly cripple basic functions, including blood transfusions, at major cancer centres such as Kenyatta National Hospital (KNH) and Kenyatta University Teaching, Referral and Research Hospital (KUTRRH).

When Auditor General Nancy Gathungu appeared before parliament in April 2025, she disclosed that MTRH, KNH and KUTRRH collectively owed suppliers Ksh7.4 billion – more than half of the Ksh14.1 billion total debt owed by all health facilities to suppliers. By September 2025, MTRH Chief Executive Dr Philip Kirwa reported a Ksh3 billion debt so severe that the hospital could only pay staff basic salaries without statutory deductions.
Dr Nyikal was pointed in his assessment of SHA: “SHA has long-lasting teething problems. Its benefit packages must be in line with the current cost of care. Delayed disbursement, slow claims approval rates and regular system downtimes must be addressed.”
He proposed consolidating all SHA funds covering cancer care into a unified framework to improve care and referral systems, noting that late-stage cancer treatment is expensive and carries low survival rates. “The cancer care situation in Kenya is that we have a bit of everything, but no framework to put them together for desired outcomes. We must look at reducing the disease burden through early diagnosis and treatment,” he said.
Cancer diagnosis should be moved to where patients are, not making them incur travel costs
Dr Ahmed Ogwell, Chief Executive of VillageReach, an NGO focused on improving healthcare access for underserved communities, argued that the fight against cancer must move beyond the clinic. “Cancer is a community affair from allocation of resources, pre-diagnosis and outcomes. We must engage the community with the correct information to ensure early diagnosis and better outcomes,” he said.

He called for Community Health Promoters and cancer survivors to lead public awareness efforts, with messages translated into local idioms and languages so they travel further. “Survivors are pillars of communicating what to avoid and the importance of early diagnosis. Diagnosis should be moved to where patients are, not making patients travel and incurring costs,” he said.
This approach aligns with the World Cancer Day 2025–2027 campaign theme, “United by Unique,” which places people at the centre of care.
The consensus from the seminar was clear: Kenya has made genuine progress in cancer financing and coverage, but without fixing diagnosis delays, reimbursing facilities on time, maintaining functional equipment and rooting cancer awareness in communities, those gains will remain out of reach for the patients who need them most.













