

For decades, Africa waited for help, reckons Prof Mohamed Janabi. Now, with the clock winding down, it is finally learning to help itself.
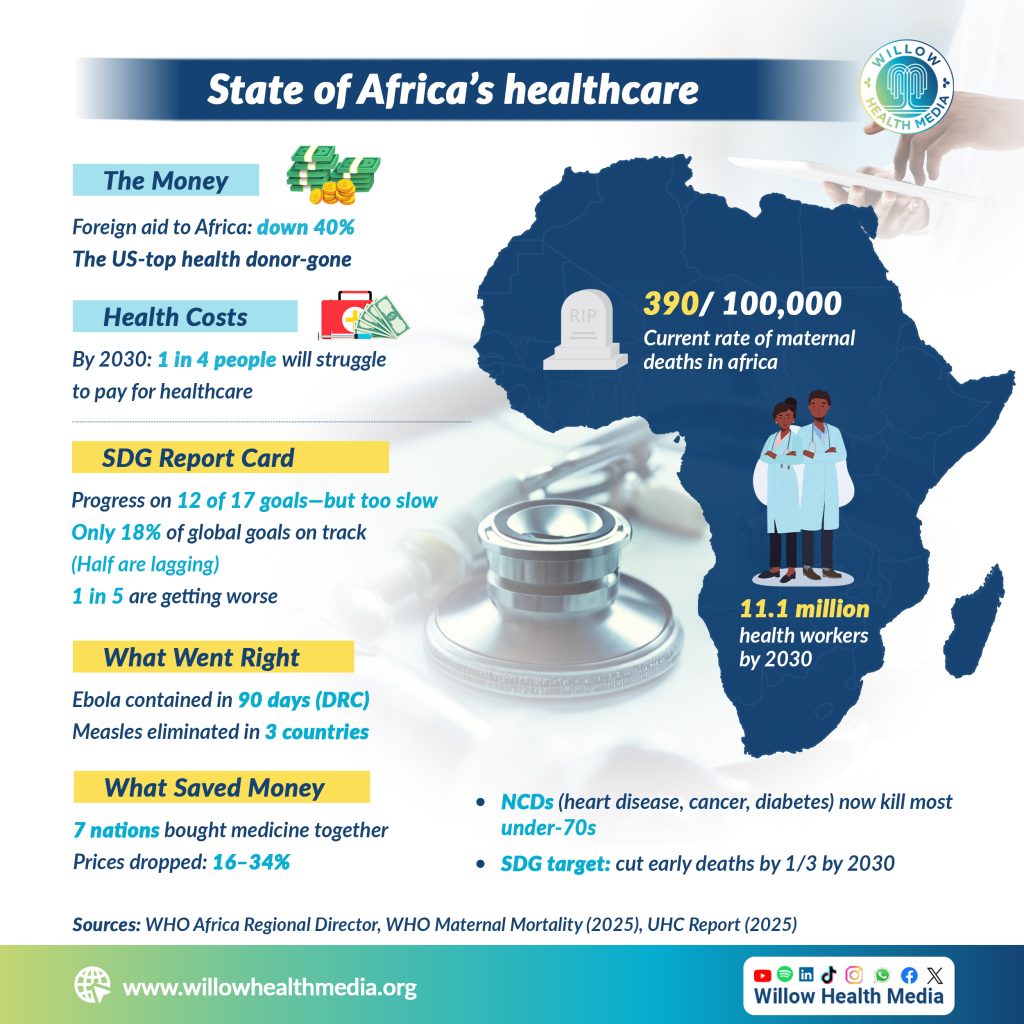
Africa is five years from its 2030 Sustainable Development Goals deadline, and the continent is falling behind. Overseas development assistance has dropped by 40 per cent. The United States – one of the continent’s biggest health donors – has pulled out entirely. And the cascading consequences are now rippling through HIV treatment programmes, malaria interventions, tuberculosis care, and maternal health services across the region.
“It has disrupted some of our gains,” Prof Mohamed Yakub Janabi, a cardiologist and the World Health Organisation (WHO) Regional Director for Africa, told Dr Mercy Korir, the Editor in-Chief at Willow Health Media.

The scale of what is at risk is staggering. Africa is making progress in 12 of the 17 SDGs, but not fast enough. On health specifically, many African countries are unlikely to meet SDG 3 by 2030 unless progress is significantly accelerated. Globally, only 18 per cent of SDGs are currently on track, with nearly half progressing too slowly and close to a fifth actually regressing.
The data is unsparing. On maternal health, current trends show that by 2030, the African region will still record 390 maternal deaths per 100,000 live births, far from the internationally agreed target of 70, according to the WHO Maternal Mortality Fact Sheet updated April 2025. Sub-Saharan Africa and Southern Asia together account for around 87 per cent of all estimated global maternal deaths.
On universal health coverage, the picture is similarly grim. Without faster progress, nearly one in four people worldwide will still face financial hardship due to health costs by 2030, with low-income countries bearing the largest gaps despite recording the fastest gains, according to the UHC Global Monitoring Report 2025.
Geopolitical tensions, climate change, antimicrobial resistance have compounded years of fragile progress
Then there is the workforce. A shortfall of 11.1 million health workers is still projected by 2030, with nearly 70 per cent of that gap concentrated in the WHO African and Eastern Mediterranean regions.
Prof Janabi acknowledges all of this, adding that geopolitical tensions, climate change, and the rising threat of antimicrobial resistance have compounded years of fragile progress.

Against this backdrop, Prof Janabi is careful to resist a narrative of pure crisis. He points to a series of achievements that rarely make international headlines; wins that demonstrate what African health systems are capable of when resources, coordination, and political will align.
“The continent is trying to adapt,” he said. “So, sovereignty is coming up. There is a setback, but there is success too.”
Ebola, one of the world’s most feared viral haemorrhagic fevers, was contained in the Democratic Republic of Congo in a record 90 days. Marburg virus, equally deadly, was successfully brought under control. Measles and Rubella have been eliminated in Seychelles, Cabo Verde, and Mauritius, a landmark achievement in immunisation systems that took years of investment to realise.
Funding crisis has exposed something deeper: a health system architecture that was never built to last
Perhaps most quietly significant is the pooled procurement initiative for small island developing states. By negotiating collectively, seven nations: Seychelles, Madagascar, Mauritius, Cabo Verde, Equatorial Guinea, Comoros, and one additional partner, reduced the cost of essential medicines by between 16 and 34 per cent. It is a model of African-led health financing innovation that deserves far wider attention.

The funding crisis has exposed something deeper: a health system architecture that was never built to last. For decades, disease programmes have operated in vertical silos, separate funding streams, separate staff, separate supply chains for HIV, tuberculosis, malaria, and increasingly, non-communicable diseases.
That model, Prof Janabi argues, is no longer sustainable, financially or structurally.
“We are advocating for countries to integrate those major vertical programmes like TB, HIV/AIDS. Now we are talking about putting cancer and non-communicable diseases into that framework too,” he said.
SDG target of reducing NCD premature mortality by one third by 2030 is currently off track
The urgency of that integration is underscored by a quietly accelerating crisis: premature deaths from NCDs such as heart disease, stroke, diabetes, and cancer are rising and now account for most deaths among people under 70 worldwide. The SDG target of reducing NCD premature mortality by one third by 2030 is currently off track.
The Lusaka Agenda and the Accra Reset, two continental frameworks gaining momentum, provide the policy architecture for this transformation. Both prioritise locally driven solutions, sovereign health financing, and the mainstreaming of vertical disease programmes under a unified primary healthcare structure.

While the Lusaka Agenda spelled out the problem and the solution, the Accra Reset is the commitment to make it happen. Together, they mark Africa’s clearest break from health aid dependency, at the very moment aid is fading away.
A WHO and World Bank joint report on universal health coverage confirmed that the global increase in health service coverage has been driven largely by advances in infectious disease programmes, with NCD coverage showing steady but slower improvement, a gap that primary healthcare integration is best placed to close.
If there is one phrase that anchors Prof Janabi’s entire argument, it is this.
“The most important thing – the lifeline for our continent – is primary healthcare, which will cover universal health coverage,” he said. “This is something which African countries really have to invest in.”
It is a deceptively simple prescription for an extraordinarily complex problem. But at a moment when donor funding is retreating, geopolitical uncertainty is rising, and the 2030 deadline is drawing closer with each passing month, primary healthcare is no longer just a policy preference. For millions of Africans, it is the only viable path forward.
The clock, as Prof Janabi knows better than most, is still ticking.















