
In Africa, about 800,000 lives are saved every year through immunisation. Yet despite these gains, one in five children on the continent still misses essential vaccines, with about 3 per cent – roughly 48,000 children – in Kenya alone.
As the world marks this year’s Immunisation Week, Africa’s record on vaccines tells two stories: remarkable progress over two decades, and a stubborn gap that continues to leave thousands of children, including in Kenya, without a single dose of even the most basic vaccines.
Data from the World Health Organization (WHO) shows that vaccines have saved more than 150 million lives globally since 1974, currently preventing over four million deaths each year. In Africa alone, about 800,000 lives are saved annually through immunisation. Yet despite these gains, one in five children on the continent still misses essential vaccines, a gap that exposes millions to preventable disease and death.

Speaking at a briefing on the findings of the first-ever detailed analysis on immunisation, malaria control and vaccination, Dr Mohamed Janabi, WHO Regional Director for Africa, acknowledged the continent’s significant strides.
“Since 2000, nearly 20 million measles-related deaths have been prevented, and more than 500 million African children have been protected through routine immunisation,” he said. “In 2024 alone, 1.9 million lives were saved.”
The introduction of malaria vaccines in 25 African countries marked another milestone, a development that signals progress in tackling long-standing infectious disease burdens. But Dr Janabi was equally blunt about what remains undone. “Momentum is slowing, and too many children remain unprotected.”
At the heart of that warning is a phenomenon known as “zero-dose” children, meaning those who have never received a single vaccine.
Across Africa, a handful of countries account for a disproportionate share of these children, a concentration that reflects deep structural inequities rather than isolated failures. Dr Benido Impouma, Director of Disease Prevention and Control at the WHO Regional Office for Africa, was unequivocal about what this represents.
The challenge is less about vaccine availability and more about equity and system strength
“Zero-dose is a sign of inequity in immunisation. It is also a human rights issue,” he said. “It is not acceptable in the 21st century to have children who cannot access even basic vaccines.”

These children are not randomly distributed. WHO has shifted its focus from national averages to granular, sub-national data precisely to find them, and the picture that emerges is one of concentrated disadvantage. Zero-dose children are disproportionately found in remote rural areas, urban informal settlements, and conflict-affected regions where health systems are thin or absent.
The COVID-19 pandemic made a difficult problem worse. Lockdowns, strained health systems, and diverted resources drove up zero-dose numbers across the continent, reversing years of hard-won gains. Recovery has been uneven, and the most vulnerable populations remain furthest behind.
Compounding the challenge is a significant funding shortfall. When major donor support was reduced by around 40 per cent, Dr Janabi explained, it sent shockwaves through immunisation programs. “The challenge today is less about vaccine availability and more about equity and system strength,” he said.
In Kenya, the statistics illustrate exactly this tension between headline progress and hidden failure. National immunisation coverage stands at approximately 80 per cent, a figure that appears solid by regional standards. But that number conceals sharp inequalities. Coverage for the first dose of the measles vaccine reached 91 per cent in 2024, yet only 76 per cent of children received the second dose necessary for full protection.
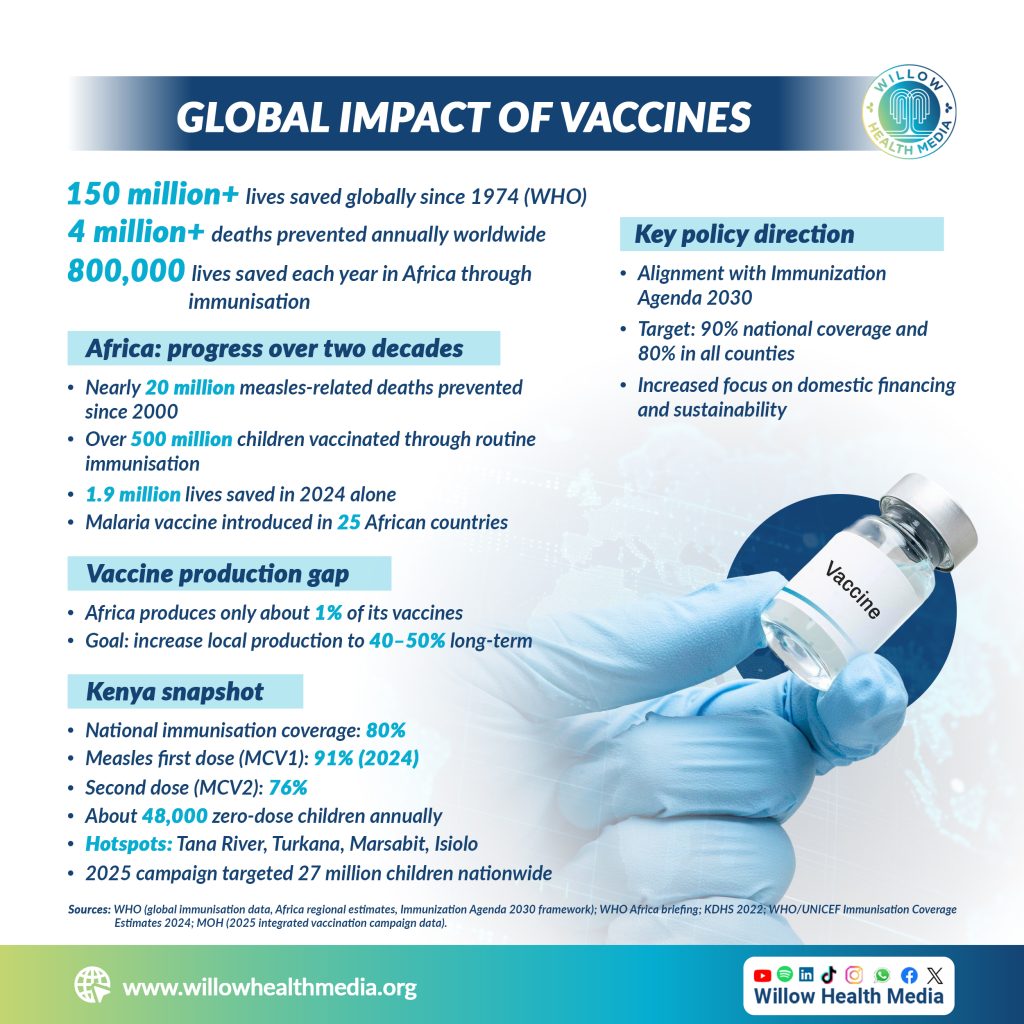
Perhaps most striking is this: data from the 2022 Kenya Demographic and Health Survey indicate that about 3 per cent of children (roughly 48,000) annually are zero-dose. These children are concentrated in marginalised regions: Tana River, Turkana, Marsabit, and Isiolo, areas defined by geographic isolation, limited health infrastructure, insecurity, and displacement.
The Covid-19 pandemic deepened these disparities, disrupting routine services and setting back progress built over the years.

Kenya has committed to the WHO Immunisation Agenda 2030, which targets at least 90 per cent national coverage and 80 per cent in every county; a commitment that means the current 76 per cent second-dose rate for measles represents not just a statistic, but a gap in which tens of thousands of children remain vulnerable to one of the world’s most contagious diseases.
In July 2025, the Ministry of Health launched a nationwide 10-day integrated vaccination campaign targeting 27 million children, introducing the Typhoid Conjugate Vaccine into routine immunisation alongside the measles-rubella vaccine. Such campaigns are critical for closing immunity gaps, but experts are consistent that campaigns alone cannot substitute for robust routine services.
Where health systems are weak and basic infrastructure absent, vaccines are necessary but insufficient
The consequences of persistent gaps are not theoretical. Outbreaks of measles, cholera, and polio continue across parts of Africa, including in countries with functioning health systems.
Dr Marie Roseline Belizaire, Regional Emergency Director at the WHO Regional Office for Africa, explained why the numbers matter so acutely. “For measles, at least 95 per cent of the population must be vaccinated to achieve herd immunity,” she said. “Many countries in Africa are far below this threshold.”

The arithmetic of measles is sobering: one case can infect up to 18 others, making it among the most contagious diseases known. When vaccination rates drop, even modestly, outbreaks become almost inevitable. The same pattern applies to other vaccine-preventable diseases, where immunity gaps create openings for rapid transmission.
Dr Janabi pushed back against the assumption that vaccines alone can solve the problem.
“Vaccines are powerful, but they are not magic,” he said. “Cholera outbreaks, for example, are driven by lack of safe water, sanitation, and hygiene.” The point is significant: immunisation does not exist in isolation. Where health systems are weak and basic infrastructure is absent, vaccines are necessary but insufficient.
A structural vulnerability that African health leaders consistently flag is the continent’s overwhelming dependence on imported vaccines. Africa currently produces only about 1 per cent of the vaccines it uses. The Covid-19 pandemic exposed how dangerous that dependence can be: when global supply chains tightened, African countries that were already at the back of the queue faced delays that cost lives.
Without predictable financing, gains remain fragile and vulnerable to the next shock
Dr Adelheid Onyango, Director of Health Systems and Services at the WHO Regional Office for Africa, framed local manufacturing not as an aspiration, but as a necessity. “We cannot rely on long global supply chains, as Covid-19 showed us,” she said. “We need manufacturing capacity within the region.”
Efforts are underway to map existing capabilities, strengthen regulatory systems, and build an ecosystem that can support vaccine production at scale. The African Medicines Agency is expected to play a central coordinating role. However, scaling from 1 per cent to the target of 40-50 per cent local production will take sustained investment and time, and neither is guaranteed.

The path forward, WHO Africa argues, runs through primary health care.
“Outbreaks start and end in communities,” said Dr Janabi. “If we invest in community health systems and build trust, we respond earlier, save more lives, and reduce costs.” This means expanding the community health workforce, improving surveillance, and embedding vaccination in routine care rather than relying on periodic campaigns to compensate for chronic system weaknesses.
Financing is the thread that runs through every challenge. The 2017 Addis Ababa Declaration on Immunisation committed governments to increase domestic funding, but implementation has been uneven. Dr Impouma was direct: “We must ensure that countries increase domestic investment while partners such as Gavi continue to support immunisation efforts.” Without predictable financing, gains remain fragile and vulnerable to the next shock.
The overarching message from WHO Africa is that the continent stands at a crossroads. Two decades of progress demonstrate what is possible. The continued existence of zero-dose children, 48,000 of them in Kenya alone every year, demonstrates how much remains undone.
“Prevention is faster, fairer, and more affordable than cure,” said Dr Janabi. “If we invest in strong systems now, we can close the remaining gaps and ensure no child is left behind.”
In Africa, and in Kenya, the challenge is no longer scientific. It is structural, financial, and political. Until it is met, thousands of children will remain at risk from diseases the world already knows how to prevent.















