
Asymptomatic patients and climate change silently drive 70 per cent of new transmissions as the deadly disease spreads across arid regions.
Kenya will not eliminate kala-azar by 2030. A new study says the country must keep up control efforts at 90 per cent coverage for the next 10 years to end the disease by 2035.
The reason for the delay: 89 per cent of people with kala-azar show no symptoms, but cause 70 per cent of new infections. This silent spread is outpacing control efforts in Kenya’s arid and semi-arid regions.

A study titled, Towards VL Elimination in Kenya, by the Centre for Epidemiological and Modelling Approach (CEMA), found that climate change and asymptomatic patients are fueling the spread of the disease as a public health crisis.
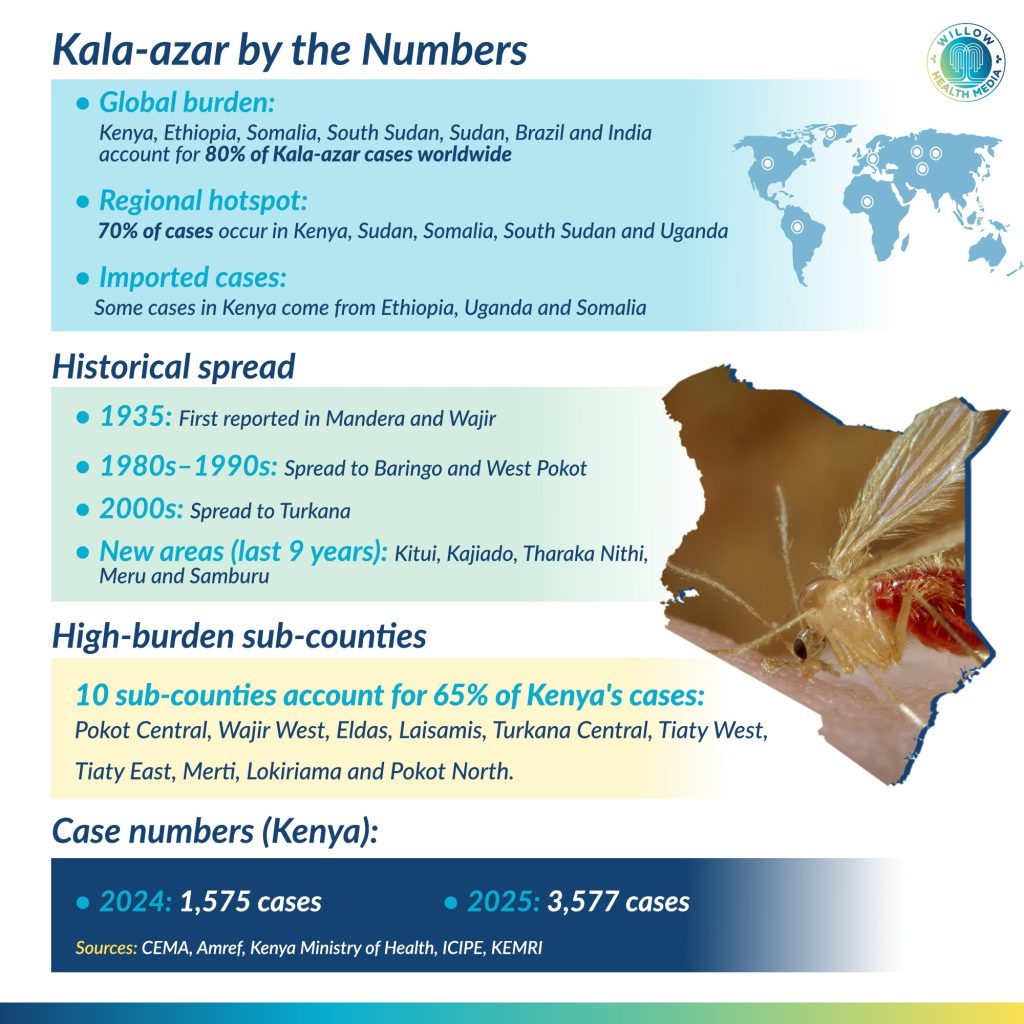
Kala-azar is spread by the bite of an infected female sandfly. The disease has killed 80 Kenyans out of 3,000 known infections in the first six months of 2025. Cases have jumped from 400 in 2011 to over 3,000 in 2025, a seven-fold rise in 14 years.
Without treatment, kala-azar kills 95 per cent of those infected. It causes fever, weight loss, and swelling of the liver and spleen. The World Health Organisation (WHO) says 73 per cent of global cases occur in eastern Africa, making the region the epicentre of the disease.
About 89% carry the disease silently, unknowingly spreading it through their communities
The study’s most alarming finding: only 11 per cent of patients show symptoms, while 89 per cent carry the disease silently, spreading it unknowingly.
“The asymptomatic contribute to 70 per cent of new infections. We must find interventions for this group,” said Dr George Omondi, a Research Fellow at CEMA.

Each infected person in a disease-free community triggers 4.87 new transmissions, a ripple effect that undermines elimination.
Annie Njanja from CEMA described kala-azar as a deadly reality exposing healthcare inequalities. She called for a shift from crisis management to sustainable elimination using data and predictive science.
“It is not just a neglected tropical disease. It’s a recurring crisis affecting the poor, with 50,000 to 90,000 cases globally each year,” she said.
The disease has carved a brutal path through Kenya’s most vulnerable communities. The study covered 22 counties, 80 sub-counties and 184 wards. It found that 13 counties battled continuous transmission between 2017 and 2025.
Kala-azar shows a cruel preference for children when they should be learning to walk, talk and play
“Turkana, West Pokot and Wajir had 68 per cent of the cases. The top five counties accounted for 86.8 per cent of the burden in Kenya. It affects the poor and marginalised most,” said Omondi.

Between 2023 and 2025, 56 wards in endemic areas became high transmission zones with over 15 cases, while 18 wards recorded mild transmission. The findings led to the stark recommendation that 33 per cent of wards needed intensive action to eliminate the disease.
The disease shows a cruel preference for the young and vulnerable. Children under 14 years constitute between 65 and 66 per cent of all patients. Twenty per cent of patients are below two years old and 17 per cent are between two and five years, ages when children should be learning to walk, talk and play, not fighting a potentially fatal disease.
Males are more prone to the disease, making up 66 per cent of cases.
“Most affected occupations were animal herders, students and self-employed individuals. Herders because they spend more time outside and are likely to get more bites,” explained Omondi.
Climate change is rewriting the map of kala-azar transmission, expanding the disease’s reach into previously unaffected areas and creating new hotspots across Kenya.
Disease transmission thrives where there are termite mounds, dung, wildlife, dogs, Manyatta housing
The study established that ecology plays a decisive role in sustaining the sandfly vector that transmits the disease. The vector thrives in arid and semi-arid areas where there are many termite mounds, vertisols (cracks in the ground), livestock dung, wildlife, dogs and Manyatta housing.
“80 per cent of Kenya is a rangeland. Ecological drivers support disease in arid and semi-arid areas. With climatic expansions, the sandflies begin to exist in new counties,” Omondi explained.
Counties like Isiolo, Meru, Kitui and Garissa now portray the same ecologies that favour sandfly existence. Bungoma’s cases have been linked to Mt Elgon’s ecological features. New areas like Narok, Samburu and Laikipia are reporting cases due to changing climatic conditions.
Grace Maina, a participant in a forum where the study findings were announced on February 4, observed that climate change played a pivotal role in the increase of kala-azar cases.
“Climate change contributes to vector dynamics. Ecological modelling is key for guiding how to mitigate risks,” she pointed out.
“Climate change plays a role; the new areas could have come on board due to the climatic changes that have been happening in the past 30 to 40 years,” Omondi explained.
Kala-azar cases peak six months into the rainy season, the disease’s incubation period, creating predictable waves of infection that healthcare systems must prepare for.
Malnutrition and HIV compound the crisis, contributing to kala-azar deaths
Kenya’s healthcare response reveals critical weaknesses that are costing lives. The treatment completion rate stands at 84 per cent, below the WHO’s recommended 90 per cent threshold. Fatality rates have increased by 3.4 per cent, a troubling trend that underscores the urgency of the crisis.

While treatment takes 17 days and patients should commence treatment within 30 days of symptoms, 24.5 per cent of Kenyans, nearly one in four, do not reach the hospital in time. The consequences are often fatal.
Malnutrition and HIV compound the crisis, with both conditions contributing to kala-azar deaths. Researchers have recommended integrating nutritional and HIV testing services into the elimination model to address these interconnected health challenges.
The projections paint a sobering picture of what lies ahead if current efforts falter. If detection, treatment and vector control efforts remain below 40 to 60 per cent, kala-azar cases will surge to 25,000 in 10 years and to 4,700 in 2030.
However, transmission can be reduced by 50 per cent if an integrated model of treatment and prevention is sustained at between 60 and 80 per cent in the next five years.
Interventions must prioritise treatment and prevention in high-burden counties-Turkana, Wajir, West Pokot
“Elimination within five years is not yet achievable now. If a kala-azar patient is introduced in a community without the disease, they cause an average of 4.87 new transmissions. We must prioritise addressing asymptomatic cases,” the researcher proposed.

“At 80 per cent coverage, we’ll still have between 1.6 and 1.8 cases per 15,000 people in Kenya. At 85 per cent, we’ll eliminate 50 per cent of the cases by 2030,” Omondi analysed.
The target is to reduce kala-azar cases to less than one in 15,000 people to ensure no further transmissions- a goal that requires sustained political will, adequate funding, and coordinated action across multiple sectors.
Researchers have predicted that Kenya will need to sustain integrated awareness, prevention, treatment and surveillance coverage at 90 per cent for the next 10 years to completely eliminate kala-azar.
Interventions must prioritise treatment and prevention in high-burden counties-Turkana, Wajir, West Pokot and Mandera-along with Isiolo and Marsabit, which have shown worrying upward trends.

Bangladesh became the first country to completely eliminate kala-azar in 2023
Spraying of insecticides and use of treated nets are key in containing indoor bites. “We need integrated vector management where we have livestock, dogs and hyraxes,” Omondi proposed.
Mary Gicheru, a participant, raised an important question about whether dogs could transmit the disease to humans since they are prone to canine leishmaniasis.

“Studies found that dogs are primary reservoirs or carriers of leishmaniasis, though they cannot transmit it directly to humans through bites, saliva or contact. A parasite must be involved. We need more studies for a solid conclusion,” Omondi explained.
Bangladesh became the first country to completely eliminate kala-azar in a certification made by the WHO in October 2023, proving that elimination is achievable with sustained commitment and comprehensive interventions.
Kenya can follow this path, but only if coverage is maintained at between 60 to 80 per cent by 2030 and 90 per cent for 10 years thereafter. The alternative-a surge in cases, more deaths, and continued suffering in Kenya’s most marginalised communities- is unacceptable.
CEMA’s study was conducted in partnership with The Gates Foundation, Amref, the Ministry of Health, the International Centre of Insect Physiology and Ecology (ICIPE) and the Kenya Medical Research Institute (KEMRI).
Graphics by Brian Wekesa.















