
Community Health Promoters (CHPs) are in all 47 counties, but unlike in rural areas, many urban residents do not know where to go for primary healthcare.
Clad in a fluorescent blue reflector jacket, black boots and carrying a red Ministry of Health bag, Ogla Serem climbs a muddy, slippery road in Kapchebar village, Elgeyo Marakwet. Rain, fog, heat or dust hardly deter her. This is routine.
Serem is a Community Health Promoter (CHP), part of Kenya’s primary healthcare system, tasked with delivering preventive, promotive, curative and rehabilitative care at the household level.

On this February morning, she’s heading to the home of Nancy Kiplagat, 28, who is expecting her third child. Her job is simple but critical. She is to confirm that Kiplagat attended her final antenatal clinic, check her blood pressure and sugar levels and ensure she’s ready for a safe delivery.
Kiplagat welcomes Serem, her purple antenatal clinic book in hand. “I am in charge of 96 households,” she tells Willow Health Media. “Today I’m following up on mothers who recently delivered and those close to delivery.”
Her goal is clear. Every mother delivers in a health facility, attends all eight antenatal visits, and eats well. Kiplagat says the visits changed how she prepared for childbirth. “The doctor taught me danger signs, how to eat well, and even spoke to my husband about supporting me.”
In villages, CHPs are trusted and visible. Residents refer to them as ‘doctors’
Kiplangat planted traditional vegetables and expanded her poultry flock to improve her diet and income.
A kilometre away, another patient, Michael Kipkemoi, waits. He suffered polio as a child and later a stroke and struggles with mobility. Serem checks his blood pressure and sugar levels and measures his nutrition using a MUAC (Mid-Upper Arm Circumference) tape.

“In December, he was at 18 centimetres, which showed poor nutrition. Now he is at 21, which is normal,” explains Serem, whose visits offer Kipkemoi lifeline care. “When she refers me, I am attended to quickly,” he says.
In villages like Kapchebar, CHPs are trusted and visible. Residents refer to them as ‘doctors’ who have slowly become critical to Kenya’s push for Universal Health Coverage (UHC) under the Social Health Authority (SHA).
CHPs link households to dispensaries and health centres, ensuring early care and reducing pressure on referral hospitals, considering Kenya’s doctor-to-patient ratio stands at one doctor per 5,263 people, according to the Kenya National Bureau of Statistics. This is five times less than the World Health Organisation (WHO) -recommended ratio of one doctor for every 1,000 people.
Kenya currently has 107,000 CHPs deployed to villages across all 47 counties since October 2023. Each CHP is equipped with a smartphone and a kit containing basic screening tools: Smartphone, MUAC) tape, weighing scale, thermometer, first aid box, blood pressure monitor and glucose testing kits.
On paper, the system is designed to bring care closer, but on the ground, the reality is different
By February 2024, these CHPs had reached 2.7 million households, with over 1.56 million Kenyans screened for diabetes and more than 1.1 million screened for hypertension, according to data from the Kenya Yearbook Editorial Board.

On paper, the system is designed to bring care closer to people. On the ground, the reality is uneven. While Kenyans in rural areas are familiar with CHPs, the same is not the case with urbanites.
In Eldoret, interviews with residents, including teachers, reveal that most haven’t had quotable encounters with CHPs or where to find primary healthcare services, let alone what is covered.
Tabitha Wacika, a food vendor along Uganda Road, says she has never met a CHP and “I don’t know which services are free and which we pay for.”
Wacika seeks care at Moi Teaching and Referral Hospital (MTRH), a level six facility where she has paid for X-rays and CT scans. She describes the discharge process under SHA as long and frustrating.
The most common problems were lack of medicines, long wait times, unaffordable costs
Others echo the confusion. Like Salina Koech, a teacher in Uasin Gishu, who says she stopped visiting her local dispensary due to frequent drug shortages, as most times, “You are told there are no drugs and given a prescription to buy outside.”

Despite being registered under SHA, she prefers private care.
Her frustration is not unusual. Among Kenyans who sought care at a public clinic or hospital, a majority say it was difficult to obtain services, with the most common problems being a lack of medicines, long wait times, unaffordable costs, and absent personnel, according to a 2026 Afrobarometer survey.
Some patients unknowingly benefit from the system.
Simon Anjichi, a resident of Kapsoya, was treated for malaria at a dispensary without paying, arguing, “I didn’t know it was free or how much the government pays.”
The lack of awareness has consequences.
Patients bypass lower-level facilities and crowd referral hospitals, paying out of pocket for services that could be accessed cheaply or free at the primary level.
Despite SHA rollout, 55 per cent of patients pay out of pocket for medical expenses
Kenyans spend about Ksh150 billion in out-of-pocket healthcare payments each year, according to the Parliamentary Budget Office, where the Health Committee notes that for every Ksh100 spent on healthcare, Ksh30 comes directly from patients’ pockets.

Jared Oyugi, a boda boda rider, understands the system better and explains that “People don’t know they should start at dispensaries. Without that, they end up paying unnecessarily.”
He points to Pioneer Health Centre, where malaria and flu can be treated at no cost, yet many patients still flock to referral hospitals.
Despite the rollout of SHA, 55 per cent of patients still pay out of pocket for medical expenses, and only one in five health facilities consistently receives government payments and reimbursements, as per a survey by Afrobarometer.
When facilities aren’t reimbursed, drugs run out, staff aren’t paid, and patients are turned away or charged. Even when the problem is known, supplies still fall short. Stockouts force patients to buy medicine from private chemists.
CHPs operate under pressure, across difficult terrain with limited resources
Some residents accuse CHPs of inconsistent engagement, saying visits increase only when supervision is expected.
At the same time, CHPs themselves operate under pressure, covering dozens of households across difficult terrain with limited resources. The co-financing model, where counties contribute half of each stipend, has also proven uneven, with some counties slow to fulfil their obligations.

Village elder Anne Chelagat believes more should be done as CHP numbers “Should be increased and they should be paid well. They are the ones helping us stay healthy.”
The government funds primary healthcare through a capitation model, paying Ksh900 per person annually for outpatient services at level 2, 3 and some level 4 facilities.
In the 2025/2026 financial year, Ksh13.1 billion was allocated to primary healthcare – nearly double the Ksh7.1 billion set aside the previous year – as part of a broader Ksh138.1 billion health budget, the largest in the country’s history as per National Treasury’s Budget statement for 2025/2026.
For every Ksh1 invested in community health, Ksh9.40 in economic and societal benefits is generated
CHPs earn a monthly stipend of Ksh5,000, split equally between the national and county governments. In February 2024, the government released Ksh3 billion to kick off the payment programme, the first time CHPs were being formally compensated.
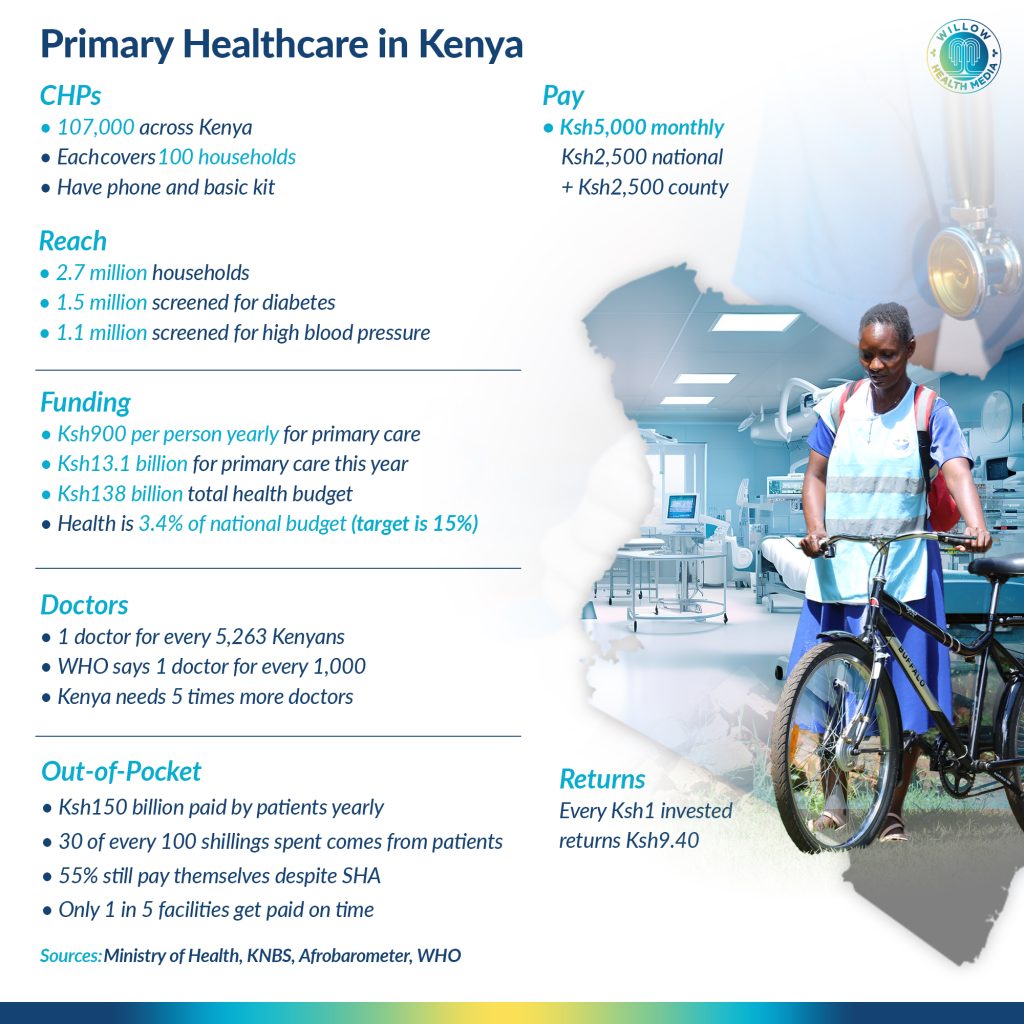
Development partners estimate that for every Ksh1 invested in community health, Ksh9.40 in economic and societal benefits is generated, according to Financing Alliance for Health. Such a return makes the case for expanding the programme far stronger than the current investment reflects.
Kenya’s health spending, meanwhile, remains well below global benchmarks.
Back in Kapchebar, Serem continues her rounds, moving from one household to the next. Her work reflects what primary healthcare is meant to be: local, preventive and continuous.
But beyond rural hills, the system begins to thin out. In towns and peri-urban settlements, awareness fades, services become inconsistent, and patients drift toward costly care.
Indeed, while Kenya’s primary healthcare model promises care at the first point of contact, for some, that promise depends on where they live.













