
Parents demanding more information and honesty from the government before letting their children be vaccinated.
Sisa Juma was appalled when his child came home from school in Lugari constituency and casually mentioned being injected that day. The parent had not consented to the typhoid vaccination administered during Kenya’s July 2025 campaign targeting 21 million children aged nine months to 14 years.

“I questioned why the school consented to my child getting the typhoid vaccine. After failing to resolve the stalemate with the school, I filed a formal complaint at the County Education Office and County Health Department,” Juma told Willow Health Media.
His frustration reflects growing vaccine hesitancy across Kenya, where parents increasingly question government health campaigns and demand greater transparency before consenting to their children’s vaccination.
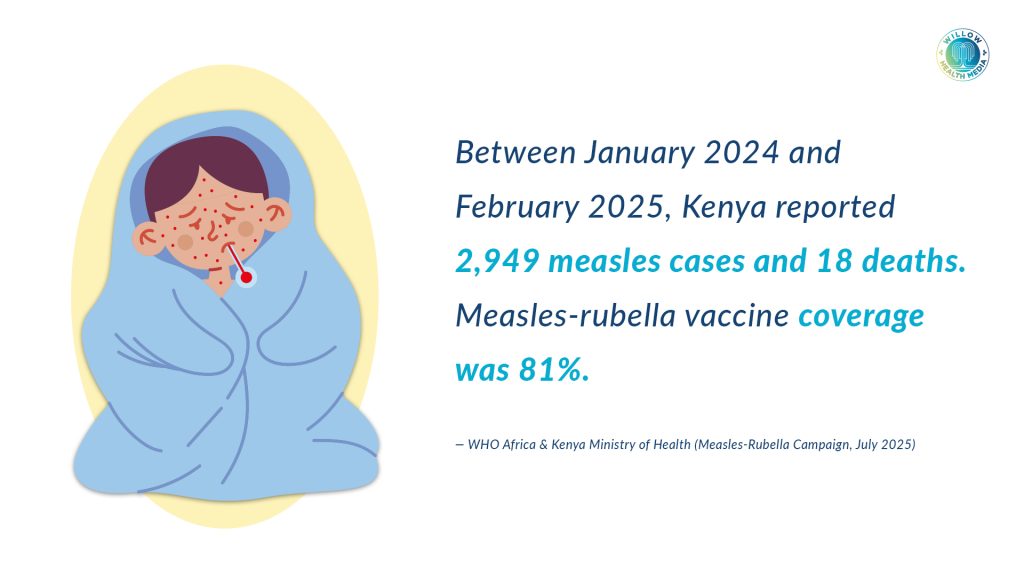
When UNICEF Kenya assured parents on Facebook that the Measles Rubella and Typhoid vaccines administered between 5-14 July 2025 were “tested and safe,” many remained unconvinced.
“As parents, many of us lost trust in the government, especially when it comes to the health and safety of our children. This sudden vaccination campaign across the country has raised serious concerns. There has been very little public awareness or proper communication. We feel left in the dark,” commented Paul Parmuya.
I have stood my ground that no jabs…when did schools become medical facilities?
Muthoni Muhu, another parent, questioned the typhoid vaccine’s necessity: “What exactly does the typhoid vaccine do when the disease is easily preventable through observing good hygiene, taking clean water and food?”
Several parents actively refused consent. “My kids’ school gave a paper for parents to give consent, but I have always stood my ground that no jabs in school,” stated Suzanne Korandu. Rosalyne Wachira asked pointedly: “When did schools become medical facilities?”

The Sozo Church of God publicly challenged Health Cabinet Secretary Aden Duale over the typhoid vaccine on 3 July 2025, posting on Facebook: “Typhoid! One of the most treatable conditions and easy to avoid na usafi [with cleanliness] and clean water?”
This religious opposition carries significant weight. Kenya’s churches provide 21 per cent of healthcare services and wield considerable influence over congregants’ health-seeking behaviours. The Sozo church had previously opposed COVID-19 vaccines and challenged the government to list typhoid deaths, questioning whether the vaccination was necessary.
Dr Wahome Ngare, a gynaecologist and Catholic Doctors Association member, has strongly opposed the HPV vaccine, linking it to infertility cases and influencing many church members’ perceptions.
There was a Catholic priest who did not allow us to conduct vaccinations in two schools
Healthcare workers encountered this hesitancy firsthand. Prof Faith Okalebo, a University of Nairobi pharmacology researcher, described her experience during the July measles catch-up immunisation campaign.

“There was a Catholic priest who did not allow us to conduct vaccination in two schools. Also, private schools were very hesitant to allow us to get in,” she disclosed during an August 2025 stakeholders forum.
Dr Evans Kiprotich, Uasin Gishu County Director of Health, confirmed that religious and cultural beliefs increasingly impede vaccination efforts.
“Lack of awareness, religious and cultural beliefs are a barrier towards attaining over 90 per cent vaccine coverage. In Uasin Gishu, the acceptability rate is at 82 per cent, though trends are changing and hesitancy is common in vaccines outside childhood immunisation schedules,” he explained.
The hesitancy stems partly from COVID-19 vaccine experiences. In 2021, Kenya’s Ministry of Health announced that 840,000 COVID-19 vaccine doses had expired due to poor uptake, attributed to “misinformation and rumours around infertility issues.”
We must reduce room for speculation by pre-empting questions and negative perceptions
Dr Bernard Awuonda, a Kisumu-based paediatrician, identified misinformation as a major barrier: “We must reduce room for speculation by pre-empting questions and negative perceptions before rolling out vaccination campaigns. It’s concerning that factual news spreads slower than misinformation.”

The Human Papillomavirus vaccine faces particular resistance despite its effectiveness against cervical cancer, which kills 5,000 Kenyan women annually. The vaccine targets girls aged 10-14 years, though boys can also receive it.
Dr Bonventure Ameyo, Deputy Director of Medical Services in Turkana County, defended vaccines as “one of the biggest and most impactful inventions in human health,” arguing that free vaccination could prevent expensive cancer treatment twenty years later.
“Rumours around HPV causing sterility are unfounded. High-income countries like Australia give to boys, but we are targeting girls first because that’s where we achieve the highest impact quickly in Kenya,” he explained.
Kenya is shifting from two HPV doses to a single-dose policy, with Ameyo noting that one dose is equally effective.
Most parents don’t understand vaccine costs and therefore undervalue them
Health authorities target schools because teenagers rarely visit health facilities. “Girls at that age are healthier and hardly seek medical services where they can access information about HPV vaccines,” Ameyo explained.
However, this strategy increasingly conflicts with parental authority expectations. Juma argued that “school administrators and teachers cannot substitute parents’ jurisdiction to give or deny consent for vaccination unless it’s an emergency.”
He demanded proper communication, parental consent forms, and transparent dialogue between stakeholders.

Dr Julia Songok, Dean of Medicine at Moi University, identified another problem: parents don’t understand vaccine costs and therefore undervalue them.
“I recently asked parents if they knew the cost of vaccinating their children in the first two years, and they said it was free. When we break down the cost the government and donors incur, then parents will respect and value vaccines,” she stated.
Parents are demanding greater transparency and proper consent procedures
Kenya allocated Ksh4.6 billion for vaccine procurement in the 2024/2025 budget, demonstrating significant government investment in immunisation programmes.
Authorities are adapting strategies to improve uptake. Kenya has reduced measles rubella vaccine doses from 10 to five to encourage compliance and prevent children from skipping schedules.
Director General of Health Dr Patrick Amoth has repeatedly assured parents about vaccine safety, particularly during October 2024’s polio and measles campaigns in nine counties.
“The vaccines have been tested and proven safe, and we have the Vaccine Safety Advisory Committee to guarantee safety and address any doubt or concerns,” he stated.
The tension between public health imperatives and parental rights continues to challenge Kenya’s vaccination programmes. While health officials emphasise vaccine safety and necessity, parents demand greater transparency, proper consent procedures, and respect for their decision-making authority.
As Prof Okalebo noted, there’s an urgent need to counter misinformation while safeguarding vaccine integrity. Success will likely depend on building trust through transparent communication, respecting parental concerns, and leveraging influential community leaders, including religious figures, to support evidence-based health messaging.
The stakes are high: achieving Kenya’s target of over 90 per cent vaccine coverage requires addressing legitimate concerns while combating misinformation that threatens public health gains.















Awareness creation is not treated with the seriousness it deserves in this country. Leaders wake up one day and decide on behalf of all other Kenyans, hadi kwa mtoto wako! Sad😔