Switching from 10 to 5 vaccines is meant to save vaccines, boost uptake and counter vaccine hesitancy.
Kenya is moving from a 10-dose to a five-dose Measles-Rubella (MR) vaccine to cut wastage and improve coverage. The move follows 2,949 measles cases and 18 deaths reported between January 2024 and February 2025.
This switch was recommended by the World Health Organization (WHO) based on studies in Zambia and Gambia as a way to boost uptake, ensure equity and counter vaccine hesitancy.

For Kenya to shift from the 10-dose to the 5-dose MR vaccine, the National Vaccination and Immunisation Programme (NVIP) needs local evidence to guide policy. During a virtual stakeholders’ forum on August 28, 2025, a study team announced it had begun a baseline survey in three counties to gather data for the policy review.
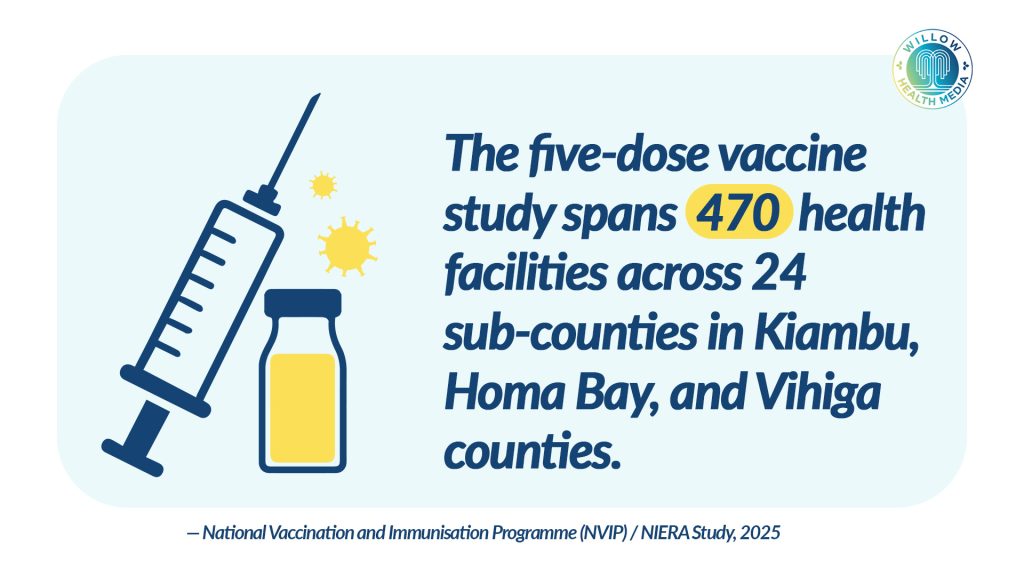
Prof Apollo Maima of Maseno University, the lead investigator, said the study is being conducted in Homa Bay, Kiambu, and Vihiga across 24 sub-counties.

It covers about 470 health facilities offering routine immunisation. Baseline data collection started in June 2025 and will run until September 30, 2025.
“We are studying 24 sub-counties where 12 will be controlled and another 12 intervention groups. The government has already procured 35,000 vials of the five-dose vaccines at an estimated cost of Ksh40 million for the investigation,” Maima stated.
The procured five-dose vaccines will be used in health facilities under the intervention group, while the 10-dose vials will continue in facilities under the control group. Control counties will not be notified and will continue with the current 10-dose vials.

Kenya recorded nearly 3,000 measles cases and 18 deaths since January 2024
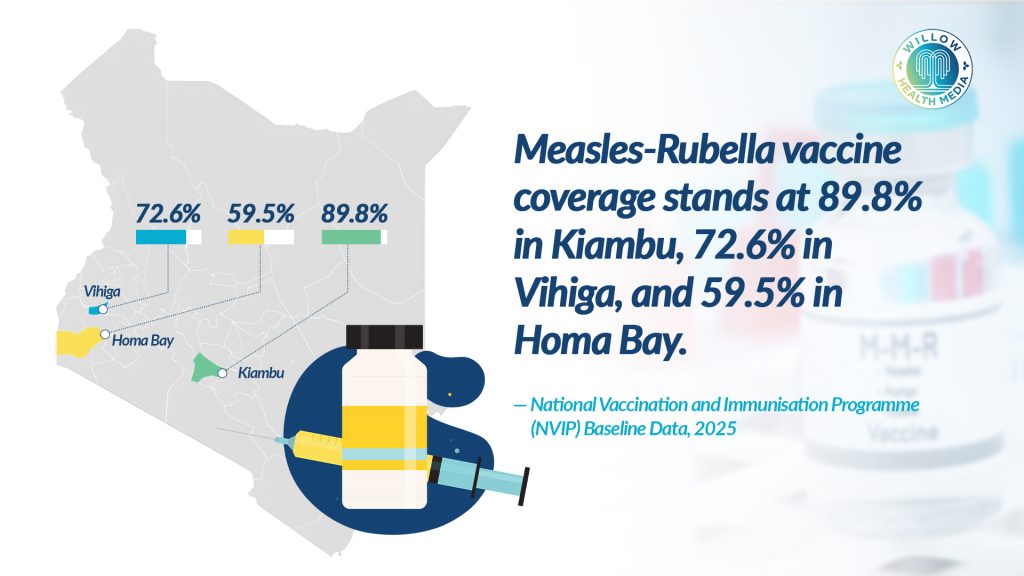
Vihiga county has 72.6 per cent, Homa Bay 59.9 per cent, and Kiambu 89.8 per cent MR vaccine coverage, with Health Cabinet Secretary Aden Duale raising concerns over low uptake of the second M-R dose, which targets children between nine and 59 months.
“Between January 2024 and February 2025, Kenya recorded nearly 3,000 measles cases and 18 deaths. This campaign is our opportunity to close that gap,” Duale said.

This study is focused on solving the major problem of many MR vaccines being thrown away, wasting money and doses, as health workers shun opening a large vial of vaccine (with 10 doses) unless they’re sure of finding 10 children to vaccinate within six hours. Or else, the leftover vaccine must be discarded.
Fear of vaccine wastage is thus preventing children from getting vaccinated, leading to “missed vaccination opportunities,” explained Prof Maima. “We want to establish if the five-dose option will encourage nurses to open vials and vaccinate children without fearing they’ll cause wastage.”
Low health workers’ motivation and confidence missed opportunities for vaccination, and increased vaccination dropout cases due to frustration by caregivers contribute to low vaccine coverage.
Changing vaccine’s packaging too much might lead to vaccine hesitancy
Dr Gladys Mooka, speaking for the nursing team, argued that the switch to five-dose vials would solve the problem as “Caregivers won’t have to pool 10 children for the vaccines to be administered, mothers won’t have to return another day for the vaccination, thus saving transport costs to the hospital.”
Dr Emily Naiseria, touching on regulation, told the vaccine program (NVIP) that they need to formally submit paperwork to the pharmacy board (PPB) to approve the new 5-dose vaccine vials with justification for how the change will “reduce wastage and enhance compliance” without impacting quality, safety, efficacy and integrity of the vaccine.
Dr Naiseria also suggested the need for training health workers on documenting vaccine details like batch numbers and expiration dates, besides tackling pollution, as using more vials leads to more physical waste and the government should address disposal challenges.
Prof Faith Okalebo, a Pharmacologist at the University of Nairobi, advised against changing the vaccine’s packaging too much, as a major redesign might lead to vaccine hesitancy, as “Significant packaging change would insinuate a change in quality, while in reality the antigen quality hasn’t been downgraded.”
Dr Supa Tunje, representing the Kenya Paediatrics Association, said that end users should be reassured that the quality and composition of the vaccine will remain the same and thus need to “involve religious groups as their views are vital.”
Negative news spreads faster, and media will be useful to counter misinformation
Dr Bernard Awuonda, a paediatrician in Kisumu, concurred, reiterating the importance of preempting negative perceptions and countering them lest misinformation about the switch goes against the MR vaccine.

“There’s a lot of negativity around contraceptives, and these narratives are used to discredit vaccines. Negative news spreads faster, and we’ll need to leverage the media to counter misinformation,” the paediatrician said.
The workload for administering the five-dose vaccine has been found to be the same as that of the 10-dose, but there were calls to increase cold chain transportation capacity due to the bulkiness of the five-dose vials.
About 27 enumerators, 11 from Kiambu, nine from Homa Bay, and seven from Vihiga have been enlisted, and a module to train 269 health workers on MR vaccination, vial usage, safe handling of vaccines, cold chain management and wastage reporting has been developed.
Purity Kiunga from the Kenya Biovax Institute disclosed that they are finalising setting up technology systems and will commence manufacturing in 2026, further lowering the cost of vaccines and ending stockouts.
The study’s findings are expected to be out in eight months, with the investigative team assuring it will share the results with all stakeholders.