
Too many girls miss the HPV vaccine in Kenya over transport costs, long clinic queues, missing school or work all worsened by myths that it leads to infertility, early sex.
Working in the public health sector has opened my eyes to many desperate situations. I have walked alongside families grappling with hunger, watched children battle diseases that science defeated decades ago, and listened to mothers’ bargain with fate at overcrowded clinics.
But nothing has shaped my understanding of health injustice more deeply than cancer, particularly cervical cancer, which is preventable, yet continues to devastate women in poor countries.

Cervical cancer is not only professional. It is painfully personal.
In 2016, I lost a friend to cervical cancer. At 34, she was young, full of plans and hopeful until the end. I remember the long hospital corridors, hushed conversations, hope thinning as treatment options narrowed. At the time, I did not yet have the language of “health systems failure” or “preventable mortality.” I only knew someone I loved was dying from a disease that should not have taken her life.
Seven years later, in 2023, cancer reared its head again-this time closer, heavier, unbearable.
I spent nights shuffling, clutching hope with both hands
My brother, two years younger, fell ill. Maxim Obwiri was like a twin. We grew up together. When cancer struck, I spent days and nights shuffling between Kenyatta National Hospital and Texas Cancer Centre in Nairobi, clutching hope with both hands.
Dr Catherine Nyongesa, the lead oncologist, was candid with us on Maxim’s chances of survival. Hope is fragile. Maxim died at Thigio Hospice in Kikuyu, which had become his and our new home too. Losing him broke something in me that statistics never could.
These losses changed how I see every girl, mother, and every missed vaccine opportunity. Cancer stopped being an abstract public health burden. It became a thief with a face.
Working with the US-funded DREAMS program in 2018 provided me with a chance to design a health program targeting adolescent girls and young women. That was how I met Hellen*, who at 13 had dreams of being a teacher.
She lives with her mother and two younger siblings in Kibra, Nairobi’s largest informal settlement, where tin-roofed shacks stretch endlessly across a maze of muddy alleyways from where her worn-out sandals slap against dirt roads on her way to school. Her uniform is clean but faded, carefully washed the night before.
Behind her bright smile lies a silent risk.
Women’s lives end not because science failed, but access did
Without access to full HPV vaccination, Hellen is vulnerable to cervical cancer, which kills nearly 70,000 women annually in sub-Saharan Africa, according to the World Health Organization (WHO).

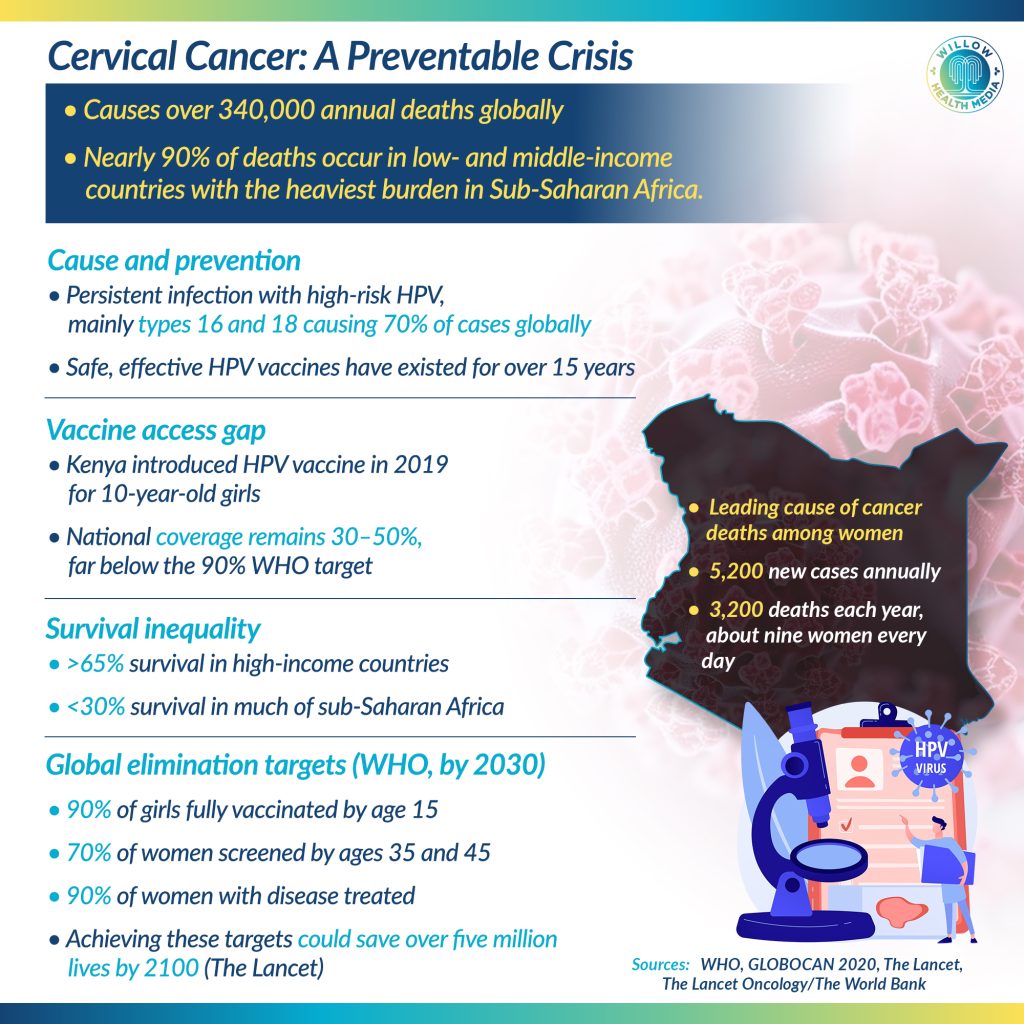
In Kenya, cervical cancer is the leading cause of cancer deaths among women. Data from GLOBOCAN 2020 shows that more than 5,200 Kenyan women are diagnosed annually, and about 3,200 die: roughly nine women every single day.
These women are not numbers. They are like my friend. Like my brother’s caregivers, who quietly told me, “We’ve done all we can.” They are women whose lives end not because science failed but because access did.
Cervical cancer is caused by persistent infection with high-risk strains of the human papillomavirus (HPV), particularly types 16 and 18, which account for nearly 70 per cent of all cases globally. Safe and effective vaccines have existed for over 15 years. In high-income countries, HPV vaccination is often delivered through schools, long before girls become sexually active. The results are extraordinary.
Sub-Saharan Africa contributes the least to global HPV vaccine coverage
A landmark study in The New England Journal of Medicine found that women in England who got HPV jab at 12–13 years saw an 87 per cent reduction in cervical cancer rates. Australia, with vaccination coverage above 80 per cent, is on track to eliminate cervical cancer in the next two decades.

Yet globally, cervical cancer still kills more than 340,000 women every year. According to WHO, nearly 90 per cent of these deaths occur in low- and middle-income countries. Sub-Saharan Africa carries one of the heaviest burdens despite contributing the least to global HPV vaccine coverage. This is not biology. It is an inequality.
Kenya introduced the HPV vaccine into its national immunisation schedule in 2019, targeting 10-year-old girls. It was a milestone celebrated by policymakers and health advocates alike. But the implementation has been uneven.
According to UNICEF and Kenya Ministry of Health reports, national HPV vaccine coverage has hovered between 30–50 per cent, far below the 90 per cent target recommended by WHO for elimination.
In informal settlements like Kibra, coverage is often lower. Barriers are layered and relentless: Transport costs to clinics, Long queues and understaffed facilities, lost wages for caregivers, School absenteeism, and Persistent misinformation

“I heard the injection makes girls infertile,” Hellen’s mother admits quietly. “Others say it encourages early sex.”
Misinformation spreads faster than facts, especially where trust in health systems is fragile. Studies in The Lancet Global Health confirm that vaccine hesitancy fueled by rumours and fear remains a major obstacle to HPV uptake across Africa. Yet fear often coexists with memory.
“I lost a cousin to cancer,” Hellen’s mother adds. “She was only 32.” I have heard this sentence too many times. I have lived it.
In Kibra, survival demands constant negotiation. Families live on a few dollars a day. Food prices rise faster than wages. School fees compete with rent. Preventive healthcare, especially for a disease that may appear decades later, feels like a distant abstraction.
Even when the vaccine itself is free, the cost of access is not.

Globally, HPV vaccines are considered cost-effective. Through Gavi, the Vaccine Alliance, low-income countries can access doses for just a few dollars. But health budgets are thin. Governments juggle malaria, HIV, tuberculosis, maternal mortality and now post-COVID recovery. Meanwhile, treating advanced cervical cancer is devastatingly expensive. A World Bank analysis shows that prevention costs a fraction of late-stage treatment, which often involves radiotherapy machines, yet some African countries have only one radiotherapy unit for millions of people.
I saw what late-stage cancer looks like, not in a report, but in hospice rooms. Pain. Waiting. Silence.
Hellen’s story could have ended like so many others. But it didn’t-this time. With the support of a community health worker- the DREAMS Mentors, she received her first HPV shot at a local clinic. The queue was long. Her mother missed a day of work. The clinic was crowded. But Hellen got vaccinated.
“She was brave,” her mother said, smiling. “She didn’t cry.”

That small vial administered in minutes may one day spare her from the corridors I walked, from the hospices I learned too well, from the grief that reshaped my life.
Cervical cancer is not just a health issue. It is a gender justice issue. Women bear the burden of a disease linked to poverty, silence, and limited autonomy. On average, women delay care due to a lack of money, permission or information, with most reaching the hospital when it’s too late.
Women most at risk of cervical cancer are those facing poverty, gender inequality and poor access to healthcare. Globally, the disease disproportionately affects women in low- and middle-income countries, where nearly 90 per cent of deaths occur, according to the WHO. Risk is highest for women who were never vaccinated against HPV, miss regular cervical screening, or live where health systems are weak.
In sub-Saharan Africa, women living in informal settlements, rural areas, or humanitarian settings face elevated risk due to delayed diagnosis and limited treatment options. Biological vulnerability is compounded by social factors: early sexual debut, early marriage, multiple pregnancies and high prevalence of HIV, which increases the likelihood of persistent HPV infection and progression to cancer.
Women living with HIV are up to six times more likely to develop cervical cancer, a disparity documented in studies published in The Lancet. Age also matters. While HPV infection is common in young women, cervical cancer often strikes women between 30 and 49 years, years critical for family stability and economic survival.
Cervical cancer is most deadly not where risk is greatest, but where protection, screening, and treatment are least accessible
Survival rates tell the story starkly. According to The Lancet Oncology, cervical cancer survival exceeds 65 per cent in high-income countries but drops below 30 per cent in much of sub-Saharan Africa.
The difference is not medicine. It is access.

In 2020, the WHO launched a global strategy to eliminate cervical cancer, with three targets by 2030:
- 90 per cent of girls fully vaccinated by age 15
- 70 per cent of women screened by age 35 and again by 45
- 90 per cent of women with the disease treated
If achieved, modelling studies published in The Lancet suggest more than five million lives could be saved by 2100. But strategies do not save lives; implementation does. That means funding vaccines, strengthening primary healthcare, confronting misinformation, and treating girls like Hellen not as beneficiaries, but as rights-holders.
Access to the HPV vaccine will not solve all her problems. But it removes one deadly certainty from Hellen’s future. For girls across the world’s poorest regions, that small vial of liquid is not just a vaccine. It is a chance. A shield. A promise.
Obwiri Kenyatta is a global health and development expert on health and gender equity, HIV, community health and climate justice.















